🚨 Go to urgent care or the ER — not a telehealth service — if you have:
- Bleeding heavy enough to soak through a pad or tampon every hour for two or more hours
- Feeling faint, dizzy, short of breath, or a racing heart with heavy bleeding
- Sudden or severe pelvic pain
- Possible pregnancy with significant pain or bleeding
- Fever and feeling acutely unwell with bleeding
Quarter-sized clots or bleeding beyond seven days are signs worth being seen for, but on their own they are not emergency criteria — they’re reasons to schedule a visit this week.
This page is for women with stable heavy perimenopausal bleeding who are researching online care options. It is not for acute bleeding or emergencies.
You called and they told you six weeks. You went online and you got a form. You’re not looking for sympathy — you’re looking for a door that opens.
Here’s what we found after reading every published price, every insurance policy, every FDA prescribing information document that applies to this symptom, and the terms of service most of these companies hope you won’t read.
AMN Healthcare’s 2025 survey put the average new-patient OB/GYN wait at 41.8 days across 15 large metropolitan markets — with a reported range of 1 to 231 days. That’s not a national average, and it doesn’t predict your wait. But it’s why you’re here, and it’s why this page exists.
The answer isn’t that telehealth solves the problem. It’s that telehealth does the part that doesn’t require a room — and then points you precisely at the part that does.
The 10-second comparison
| Who you are | Where to start | Key limit |
|---|---|---|
| Commercial PPO insurance | Midi Health | Cannot treat Medicaid/Medi-Cal even self-pay; not covered by Medicare |
| Paying cash, no OB/GYN | Sesame | In-person only in select cities; excludes Medicare, Medicaid & TRICARE |
| Medicaid, Medicare, or TRICARE | Your plan’s OB/GYN directory | Both Midi and Sesame exclude federal program beneficiaries |
| Already evaluated, need HRT | Winona (37 states) | No insurance accepted; not for undiagnosed bleeding |
| Any urgent sign above | Urgent care or ER | Not a telehealth decision |
All prices and policies verified from provider pages, July 2026. Affiliate disclosure: we may earn a commission from Midi, Sesame, and Winona links on this page. Hers and Inner Balance links go to our own review pages and earn us nothing.
What no video visit can do — and why that matters for every FDA-approved option
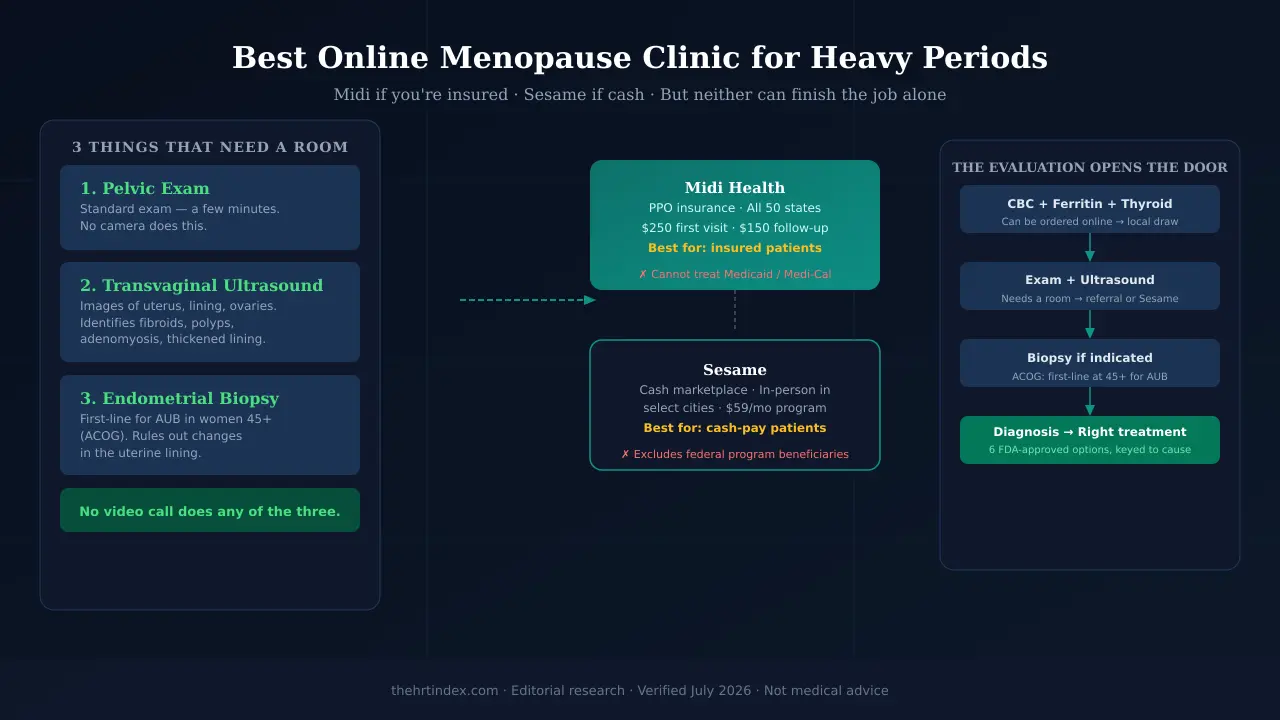
Before we name a single platform, you need to understand why this category is harder than online HRT for hot flashes. There are six FDA-approved treatments for heavy menstrual bleeding. Every single one requires something that can only happen in a room:
Pelvic exam
Standard physical exam. Takes a few minutes. No camera or microphone replaces it. Required before most treatment decisions.
Transvaginal ultrasound
Images of the uterus, lining, and ovaries. Identifies fibroids, polyps, adenomyosis, and a thickened lining. Needs a probe and a room.
Endometrial biopsy
ACOG’s first-line evaluation for abnormal uterine bleeding in women 45 and older. Rules out changes in the uterine lining. Requires a person and a procedure.
The six-product fork: Natazia (Pill) is approved for heavy bleeding with no diagnosed uterine condition. Myfembree and Oriahnn require fibroids to be present. Those are opposite prerequisites— and both come straight from the FDA labels. You cannot be sorted into the right treatment by a form. The evaluation isn’t the obstacle. It’s the map.
What telehealth cando: take a thorough history, spot warning signs in your symptoms, order bloodwork, and manage the parts of your care that genuinely fit inside a video call — while directing you precisely to the in-person pieces that don’t. That’s what separates the platforms that are worth your time from the ones that aren’t.
Check whether online care fits your situation
Take the free 2-minute matching tool →No diagnosis. No email required to see your result.
Midi Health: best for PPO insurance
Prices and policies verified from Midi’s pricing and insurance page, July 2026
Midi Health is an NCQA-accredited menopause-focused telehealth service with licensed clinicians in all 50 states. It’s in-network with many commercial PPO plans — which means your visit may cost significantly less than the self-pay rate, depending on your deductible, copay, and coinsurance. Coverage varies by plan; confirm before you book.
For a woman with unexplained heavy bleeding, Midi’s value is this: a menopause-trained clinician takes your history, orders the bloodwork that can be done remotely, and states that it refers out to an OB/GYN when an in-person exam is needed. That handoff — with a referral and context rather than a dead end — is the thing most online services don’t do.
Midi exclusions — read these carefully
- Medicaid and Medi-Cal: Midi cannot treat Medicaid patients — not even as self-pay. This is a published policy, not a billing issue.
- Medicare: Midi is not covered by Medicare or any Medicare-related plan. Self-pay visits are possible but generate no Medicare claim.
- Insurance coverage guarantee: Being in-network doesn’t mean your specific plan covers this visit. Confirm before you book.
Before you pay Midi — ask these first
- Is your specific plan name in-network? (Not just “PPO” — the specific plan.)
- Which diagnosis and procedure codes will be submitted for a heavy bleeding evaluation?
- Is the laboratory in-network with your plan?
- Can you get a pre-service cost estimate?
- If a pelvic exam or imaging is needed, does Midi provide a referral or are you on your own?
Asking those questions before anyone draws blood is free and takes 90 seconds. Nobody at Midi is reviewing your specific plan for you.
Sesame: best for cash-pay, and the only one that sells the room
Prices and policies verified from Sesame’s service pages and terms of service, July 2026
Sesame is a cash-pay marketplace — no insurance billing on either side of the transaction. What makes it different for this page is structural: it’s the only service in this comparison that actually sells in-person appointments. In the markets where it operates, you can book gynecology visits and pelvic imaging directly, with prices shown before you commit.
That business model matters for heavy bleeding specifically. Pelvic exams and transvaginal ultrasounds can’t happen over a screen. Sesame is the one platform in this comparison that sells access to the room — not a referral to someone who sells access to the room.
Sesame limits you need to know
- Federal program exclusion:Sesame’s terms of service require users to certify they are not Medicare, Medicaid, or TRICARE beneficiaries. This is not a “you’d pay twice” situation — the service is not available to you if you are a federal program beneficiary.
- In-person services are not everywhere: Gynecology and pelvic imaging are listed in select cities only. Check your ZIP before you get attached to this lane.
- Ferritin is not in the standard lab panel:The standard Sesame lab panel includes CBC, A1c, thyroid, lipid panel, and CMP — not ferritin, and not pregnancy testing. Ferritin is the test that explains exhaustion from blood loss. Ask specifically whether it’s available and how it’s priced.
- Imaging requires an order: Sesame states that the type of ultrasound depends on what the doctor orders. Confirm the order-to-imaging workflow in your ZIP.
Why Hers, Winona, and Inner Balance aren’t the right answer here
Hers
Hers markets directly to women searching for menopause help. Its own pages do not publicly document whether clinicians evaluate abnormal bleeding, order imaging, or refer for sampling. We could not verify from public sources that it does any of those things. We have affiliate relationships with Hers and took the link off this page on purpose, because it’s not the right first stop for undiagnosed heavy bleeding. See our general provider comparison for where Hers fits.
Winona (37 states + Puerto Rico)
Winona has intake with physician review and a mixed formulary of FDA-approved and compounded products. It does not publicly document a diagnostic pathway for abnormal bleeding. It’s not available in 13 states. No insurance accepted.
The conditional case for Winona: if you have already been evaluated — you have your diagnosis, you know what you’re treating, and the result of that evaluation is that you need standard menopausal HRT — Winona is a legitimate option if it operates in your state. That’s a real person with a real need. Just not the person who typed this search.
Inner Balance / Oestra
Inner Balance’s Oestra program markets itself prominently on convenience — no lab work, no office visit. That framing is precisely what makes it the wrong answer for someone with unexplained heavy bleeding. We have a relationship with Inner Balance and took the affiliate link off this page on purpose. An undiagnosed cause requires evaluation, not a subscription that skips the evaluation.
11-provider comparison matrix
Evidence legend: ✅ Provider explicitly states it does this · ⚠️ Provider states it does, with significant caveats · ❌ Provider explicitly states it does not do this · 🔍 Not published — we could not verify
| Platform | All 50 states | Takes insurance | Video visit | Orders bloodwork | Bleeding evaluation | Pelvic exam | Imaging access | OB/GYN referral | FDA-approved Rx | Compounded Rx |
|---|---|---|---|---|---|---|---|---|---|---|
| Midi Health | ✅ | ✅ | ✅ | ✅ | 🔍 | ❌ | 🔍 | ✅ | ✅ | 🔍 |
| Sesame | 🔍 | ❌ | ✅ | ✅ | 🔍 | ⚠️ | ⚠️ | 🔍 | ✅ | 🔍 |
| Winona | ⚠️ | ❌ | ✅ | 🔍 | 🔍 | ❌ | ❌ | 🔍 | ✅ | ✅ |
| Hers | 🔍 | 🔍 | 🔍 | 🔍 | 🔍 | 🔍 | 🔍 | 🔍 | 🔍 | 🔍 |
| Inner Balance | 🔍 | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ | 🔍 | ✅ |
| Gennev | 🔍 | 🔍 | ✅ | 🔍 | 🔍 | ❌ | 🔍 | 🔍 | ✅ | 🔍 |
| Alloy | 🔍 | 🔍 | ✅ | 🔍 | 🔍 | ❌ | 🔍 | 🔍 | ✅ | 🔍 |
| Evernow | 🔍 | 🔍 | ✅ | 🔍 | 🔍 | ❌ | 🔍 | 🔍 | ✅ | 🔍 |
| Plume | 🔍 | 🔍 | ✅ | 🔍 | 🔍 | 🔍 | 🔍 | 🔍 | 🔍 | 🔍 |
| Elektra Health | 🔍 | 🔍 | ✅ | 🔍 | 🔍 | ❌ | 🔍 | 🔍 | ✅ | 🔍 |
| Ospia Health | 🔍 | 🔍 | ✅ | 🔍 | 🔍 | 🔍 | 🔍 | 🔍 | 🔍 | 🔍 |
🔍 cells are blank because these companies don’t publish the answer — not because the answer is yes or no. We’ve left them visibly blank rather than guess in either direction.
The evaluation: what gets ordered and what it finds
Before any treatment decision can be made, three categories of evaluation generally need to happen — in any combination, depending on your situation and your clinician’s judgment:
| Test / Procedure | What it answers | Can be done remotely? |
|---|---|---|
| CBC (complete blood count) | Whether you are anemic; platelet count | Yes — order online, draw locally |
| Ferritin | Iron stores (can be low even with normal CBC) | Yes — but not in Sesame’s standard panel |
| TSH (thyroid) | Thyroid dysfunction as a contributing cause | Yes — order online, draw locally |
| Pregnancy test | Rules out pregnancy-related cause | Yes — urine or blood |
| Pelvic exam | Visible structural causes, cervix, uterus size | No — in-person only |
| Transvaginal ultrasound | Fibroids, polyps, adenomyosis, lining thickness | No — in-person only |
| Endometrial biopsy | Uterine lining pathology; ACOG first-line at 45+ | No — in-person procedure |
A note on the biopsy
ACOG guidance describes endometrial sampling as a first-line test for abnormal uterine bleeding in patients older than 45 — and in younger patients with risk factors, unopposed estrogen exposure, persistent bleeding, or treatment that hasn’t worked. It’s guidance a clinician applies to your individual situation, not a rule that fires automatically at a birthday.
On pain:Pain varies widely — some people report brief cramping, others report substantial pain. ACOG’s May 2025 Clinical Consensus on pain management for in-office uterine and cervical procedures supports discussing available options and notes that topical anesthetics and pre-procedure NSAIDs may reduce pain for some patients. You’re entitled to that conversation before the procedure, not after.
The six FDA-approved treatments — and what each one requires
These are not interchangeable. Which one applies depends entirely on the cause — which is why the evaluation comes first.
| Drug (brand) | Class | Approved indication | Key prerequisite |
|---|---|---|---|
| Tranexamic acid (Lysteda) | Antifibrinolytic | Cyclic heavy menstrual bleeding | Label directs excluding endometrial pathology first; contraindicated with combined hormonal contraception |
| Levonorgestrel IUS (Mirena) | Hormonal IUD | HMB up to 5 years | Patients choosing intrauterine contraception; insertion by trained provider in person |
| Levonorgestrel IUS (Liletta) | Hormonal IUD | HMB up to 5 years (sNDA 2023) | Patients choosing intrauterine contraception; insertion by trained provider in person |
| Estradiol valerate / dienogest (Natazia) | Oral contraceptive | HMB not caused by a diagnosed uterine condition | Requires no diagnosed uterine condition — opposite of Myfembree/Oriahnn |
| Relugolix combination (Myfembree) | GnRH antagonist + add-back | HMB associated with uterine fibroids, premenopausal, up to 24 months | Requires confirmed fibroids; boxed warning; up to 24 months |
| Elagolix combination (Oriahnn) | GnRH antagonist + add-back | HMB associated with uterine fibroids, premenopausal, up to 24 months | Requires confirmed fibroids; boxed warning; up to 24 months |
About standard HRT:Standard menopausal hormone therapy — the estradiol-plus-progesterone most online clinics sell — is not FDA-approved for heavy menstrual bleeding. It’s approved for hot flashes, genitourinary symptoms, and bone loss. The four estradiol labels we read also list undiagnosed abnormal genital bleeding as a contraindication. Note the nuance: Myfembree and Oriahnn containestradiol and are approved for heavy bleeding. Estrogen isn’t the villain. Estrogen without a diagnosis is the problem.
Six products. Different prerequisites. Which conversation are you in?
Match my situation to the right starting point →Can HRT cause heavy bleeding? And is HRT birth control?
If you’re already on HRT and now you’re bleeding
Starting or changing a hormone regimen can change your bleeding pattern. Some spotting or unscheduled bleeding in the first months is common, and it often settles.
Here’s the rule that holds regardless: tell your prescriber. New, heavy, worsening or persistent bleeding gets reviewed, not waited out.
Being on estrogen doesn’t retroactively account for the bleeding. “Undiagnosed” is the word doing the work in the contraindication. If you started hormones for hot flashes and now you’re bleeding heavily, the bleeding still hasn’t been explained.
HRT is not birth control
Menopausal hormone therapy does not prevent pregnancy.And you can still get pregnant during perimenopause — twelve consecutive months without a period is the line, and until you’re past it, pregnancy is possible. Which is why, wherever pregnancy is biologically possible for you, a pregnancy test stays on the list of things to rule out.
What to say so you’re not dismissed again
The difference is almost never how insistent you are. It’s whether you bring numbers or adjectives. “It’s really heavy” is an adjective — it slides off. “I’m soaking a super tampon every ninety minutes and passing clots the size of a quarter” is data. Data gets acted on.
“I’m soaking through a pad or tampon every [X] hours and passing clots about the size of a [coin]. It’s been [X] days.”
Numbers, not adjectives. This alone changes the temperature of the room.
“I’m [age] with abnormal uterine bleeding. Does ACOG’s endometrial sampling guidance apply to me?”
You’re not demanding a biopsy. You’re asking whether published professional guidance applies to your situation. No reasonable clinician minds having that conversation.
“Can we check a CBC and a ferritin? I’ve been exhausted and I’d like to look at my iron stores.”
Both, not one. They answer different questions.
“Which diagnosis and procedure codes do you expect to submit for these? Is the lab in network, and can I get a pre-service estimate?”
The same test can land very differently depending on how it’s submitted and where it’s done. Asking before anyone draws blood is free and takes 90 seconds. Coding is not a coverage guarantee — but asking the question is the difference between finding out now and finding out later.
“If you can’t do the exam and imaging here, who can, and how fast can I get in?”
This turns a dead end into a referral. Ask it before you hang up.
Ten questions to ask before you pay anyone
These are the questions behind the 🔍 cells in our matrix above — things these companies don’t publish. Ask them yourself, before your card comes out:
- Will I get a live video visit, or a form reviewed?
- Is the clinician experienced with abnormal bleeding specifically — not menopause generally?
- Can you order a CBC and ferritin, and how are they billed?
- Can you order or coordinate pelvic imaging? Where does the order go?
- What happens if I need a pelvic exam or a biopsy — do you refer, or am I on my own?
- Who reviews my results, and when?
- Will I see the same clinician at follow-up?
- Is the medication you’d prescribe FDA-approved, or compounded?
- What’s the total: visit, follow-up, medication, labs, cancellation?
- Are you available in my state, and in network with my specific plan?
If a service can’t answer those, it isn’t your first stop for undiagnosed bleeding.
How The HRT Index chose these providers
The HRT Index Verification Standard is the documented process by which we review providers: we read every published price, separate FDA-approved from compounded, verify state availability and insurance, and re-check on a fixed schedule — top providers monthly, the full roster quarterly.
What we actually verified (July 2026):Midi Health’s pricing and insurance page. Sesame’s service pages, women’s health pages, and current terms of service. Winona’s online menopause and HRT pages. Inner Balance’s Oestra pricing. FDA prescribing information for Lysteda, Mirena, Liletta, Myfembree, Oriahnn, and Natazia. FDA-approved labeling for four named estradiol products. ACOG guidance on heavy menstrual bleeding, bleeding after menopause, endometrial sampling, and the 2025 clinical consensus on pain management. AMN Healthcare’s 2025 wait-time survey.
What we could not verify:Every cell marked 🔍. We have not enrolled with any provider, tested a checkout, timed an appointment, or verified an individual insurance plan. Where we say a provider “states” something, that means the provider states it — not that we watched it happen. What we are not: clinicians. This page organizes published information and dates it. It does not diagnose you.
Update schedule: Midi and Sesame prices, policies and terms get re-checked monthly; the rest of the roster quarterly. FDA labeling and ACOG guidance get checked annually and whenever they change.
How we make money:We may earn a commission from the Midi, Sesame, and Winona links on this page. The Hers and Inner Balance links go to our own review pages and earn us nothing — we have relationships with both and took the affiliate links off this page on purpose, because neither one is the right answer to the question you asked. The Winona link is behind a condition most readers of this page won’t meet. Full disclosure.
Edge cases: when the answer changes
I have Medicaid
Midi cannot treat you — not even as a self-pay patient. And Sesame’s terms require you to certify you’re not a federal program beneficiary, so it isn’t a cash workaround. Your route is your plan’s OB/GYN directory. Ask two specific questions: “Is there a nurse triage line?” and “Do you have a cancellation list I can go on?” Describe the bleeding in numbers — pads per hour, clot size, days, and whether you’re dizzy or breathless. Medicaid and HRT →
I have Medicare or TRICARE
Midi isn’t covered by Medicare or any Medicare-related plan. Sesame’s terms exclude federal program beneficiaries. Your route is a participating OB/GYN through your own coverage, and the same two questions above apply. Medicare and HRT →
I’m rural and the nearest OB/GYN is 90 minutes away
Bloodwork travels — do that part locally and remotely. Then make one trip count: ask whether the exam and the imaging can be scheduled the same day at the same place, and whether imaging needs an order first. That one question can save you a second 90-minute drive.
I’m already on HRT and started bleeding
Tell your prescriber. Don’t wait it out on a timeline you read somewhere. Being on hormones doesn’t explain the bleeding — it just means the bleeding is happening on hormones. Being on estrogen doesn’t retroactively account for undiagnosed bleeding.
I already have an IUD and I’m still bleeding heavily
New, heavy, persistent or worsening bleeding with an IUD in place warrants clinician review. Depending on your situation, they may want to check pregnancy possibility, infection, device position, or a structural cause.
I’ve had an endometrial ablation
Tell whoever you see, early in the conversation. A previous ablation can complicate how later bleeding is evaluated. This one specifically wants a gynecologist.
I’ve had a hysterectomy
Then this isn’t your page, and any bleeding needs a clinician regardless. HRT after hysterectomy →
I’ve gone 12 months with no period and now I’m bleeding
Not this page, and not an online HRT purchase. Prompt in-person evaluation, even if it’s only spotting. If it’s heavy or you feel faint or short of breath, that’s urgent care instead. This is the symptom that gets checked, not watched.
Can I get an IUD through an online clinic?
The prescription, potentially. The placement, no — both Mirena’s and Liletta’s labels require a trained provider to insert it, in person.
Will insurance cover the ultrasound and the biopsy?
It depends on your plan, medical necessity rules, network status, prior authorization, your deductible, where it’s done, and whether the facility and the radiologist bill separately. Get a pre-service estimate for the specific procedure at the specific facility. Ask whether the quote includes the radiologist’s reading — that’s the one that ambushes people.
Frequently asked questions
Can an online menopause clinic treat heavy periods?
Not completely, and not on its own. A telehealth clinician can take your history, spot warning signs, order bloodwork, diagnose things within the scope of that visit, and work out what has to happen locally. What no video visit can do is perform a pelvic exam, pelvic imaging, or endometrial sampling — and those are the parts that usually identify the cause.
What is the best online menopause clinic for heavy periods?
Midi Health for women with an eligible commercial PPO: it offers menopause-focused virtual care in all 50 states, is in-network with many PPO plans, and states it refers to an OB/GYN when an in-person exam is needed. Sesame for cash-pay women: it's the only service in this comparison that sells in-person appointments, listing gynecology and pelvic imaging in select markets at prices shown before booking. Midi cannot treat Medicaid patients even as self-pay and isn't covered by Medicare; Sesame's terms exclude Medicare, Medicaid and TRICARE beneficiaries.
Can a telehealth doctor prescribe anything for heavy bleeding?
Tranexamic acid (Lysteda) is FDA-approved for cyclic heavy menstrual bleeding and needs no procedure, so it's the one that can fit inside an online visit. Its label directs clinicians to exclude endometrial pathology before prescribing, and it's contraindicated with combined hormonal contraception and in people with thromboembolic contraindications. Whether it's right for you is a clinical decision, not a checkbox.
Does HRT stop heavy periods?
Standard menopausal hormone therapy is not FDA-approved for heavy menstrual bleeding — it's approved for hot flashes and night sweats, genitourinary symptoms, and bone loss prevention. Several other products do carry heavy menstrual bleeding indications, each for a specific cause or population: Lysteda, Mirena, Liletta, Natazia, Myfembree and Oriahnn. Each estradiol label we reviewed also lists undiagnosed abnormal genital bleeding as a contraindication.
What is FDA-approved for heavy menstrual bleeding?
Six products, each for a different situation. Tranexamic acid (Lysteda) for cyclic heavy menstrual bleeding. Mirena and Liletta, both levonorgestrel intrauterine systems, for up to five years in patients who choose intrauterine contraception. Natazia for heavy bleeding not caused by a diagnosed uterine condition, in patients choosing the Pill. Myfembree and Oriahnn for heavy bleeding associated with uterine fibroids in premenopausal women, for up to 24 months. They are not interchangeable, and which one applies depends on the cause.
Can HRT make bleeding worse?
Starting or changing a hormone regimen can change your bleeding pattern, and some unscheduled bleeding in the early months is common. New, heavy, worsening or persistent bleeding should be reviewed by your prescriber rather than waited out on a general timeline.
Is HRT a form of birth control?
No. Menopausal hormone therapy does not prevent pregnancy. Pregnancy remains possible during perimenopause until 12 consecutive months have passed without a period, which is why pregnancy testing stays relevant wherever pregnancy is biologically possible.
Does Midi Health take insurance?
Midi is in-network with many PPO plans; coverage varies by plan, and deductibles, copays and coinsurance still apply. Self-pay is $250 for a first visit and $150 for follow-ups, verified July 2026. Midi does not accept Medicaid or Medi-Cal and cannot treat those patients even as self-pay, and it is not covered by Medicare.
Can I book a pelvic ultrasound without a referral?
Sesame lists pelvic imaging in the markets where it operates, and states the type of ultrasound depends on what the doctor orders — so check both availability and any order requirement in your ZIP before assuming. Elsewhere, imaging generally requires a clinician's order. Cash prices vary widely, so call more than one facility and ask whether the quote includes the radiologist's reading.
Do I need an endometrial biopsy at 45 for heavy periods?
ACOG guidance describes endometrial sampling as a first-line test for abnormal uterine bleeding in patients older than 45, and in younger patients with risk factors, unopposed estrogen exposure, persistent bleeding, or treatment that hasn't worked. It's guidance a clinician applies to your individual situation, not a rule that fires automatically at a birthday.
Does an endometrial biopsy hurt?
Pain varies widely — some people report brief cramping, others report substantial pain. Ask before the appointment what pain-control options are offered; ACOG's 2025 clinical consensus supports discussing available options and notes that topical anesthetics and pre-procedure NSAIDs may reduce pain for some patients. You're entitled to that conversation before the procedure, not after.
When should I go to the ER for heavy bleeding?
When heavy bleeding comes with feeling faint, severe dizziness, shortness of breath or a racing heart; with sudden or severe pain; with possible pregnancy plus significant pain or bleeding; or with fever and feeling acutely unwell. Quarter-sized clots or bleeding beyond seven days are signs of heavy menstrual bleeding worth being seen for, but on their own they are not emergency criteria.
Why am I so exhausted with heavy periods?
Heavy blood loss can contribute to iron deficiency. In the SWAN study of 2,329 women, those with three or more heavy bleeding episodes in six months had higher odds of reporting fatigue — an association across a population, not proof of cause in any individual. A CBC can show anemia and a ferritin test measures iron stores; they answer different questions, and ferritin can be low even when a blood count looks normal.
Is heavy bleeding in perimenopause a sign of cancer?
ACOG names abnormal bleeding as a possible early sign of endometrial cancer, which is why the evaluation exists and why sampling guidance begins at 45. It is one of several possible causes, alongside fibroids, polyps, adenomyosis, thyroid problems, bleeding disorders, pregnancy and hormonal cycle changes. The test is how you find out which.
How long does it take to see an OB/GYN for heavy bleeding?
AMN Healthcare's 2025 survey reported an average new-patient OB/GYN wait of 41.8 days across 15 large US metropolitan markets, with a reported range of 1 to 231 days. That's 15 selected big-city markets, not a national average, and it doesn't predict your wait. Urgent symptoms shouldn't wait for a routine slot — call and describe the bleeding specifically, or go to urgent care.
What's the difference between compounded and FDA-approved hormone therapy?
FDA-approved products are reviewed by the FDA for safety, effectiveness and quality before marketing and carry FDA-approved labeling, including a contraindication list. Compounded products are mixed by a pharmacy, are not FDA-approved, and do not carry FDA-approved labeling. That absence doesn't mean the ingredients have no known risks — it means the reviewed document doesn't exist, and the FDA has warned that compounded labeling may omit information needed for safe use.
The bottom line
You came here for a clinic. What you actually needed was a route.
If you have PPO insurance: start with Midi. Get the history taken properly and the bloodwork ordered — and ask the billing questions before anyone draws blood.
If you’re paying cash or you don’t have an OB/GYN:check your ZIP on Sesame. If in-person gynecology and imaging are listed near you, that lane is open, and it’s the fastest honest route we found.
If you have Medicaid, Medicare or TRICARE, or any urgent sign:neither of them, and we’re not going to pretend otherwise. Your own network, and the two questions about triage lines and cancellation lists.
Either way, the three things nobody can do on a screen still have to happen. And now you know why you want them to: six different medications are FDA-approved for heavy menstrual bleeding, and every one of them is keyed to a cause. One is approved only if your uterus is clear. Two are approved only if you have fibroids. You can’t be sorted into the right one by a form.
The evaluation isn’t the toll. It’s the map.
Still not sure which HRT program is right for you?
Take our free 2-minute matching quiz →Educational only. This page and this tool do not diagnose any condition, replace individual medical care, or provide emergency services. If you’re bleeding heavily and feel faint right now, stop reading and get help.
Sources
Clinical and regulatory (primary)
ACOG, Heavy Menstrual Bleeding patient guidance — acog.org/womens-health/faqs/heavy-menstrual-bleeding
ACOG, Bleeding After Menopause Could Be a Problem. Here’s What to Know
ACOG, Pain Management for In-Office Uterine and Cervical Procedures, Clinical Consensus, May 2025
FDA prescribing information — LYSTEDA (tranexamic acid), 022430s009lbl
FDA prescribing information — MIRENA (levonorgestrel-releasing intrauterine system), 021225s043lbl
FDA prescribing information — LILETTA (levonorgestrel-releasing intrauterine system), HMB indication approved 2023
FDA prescribing information — MYFEMBREE (relugolix, estradiol, norethindrone acetate), 214846s012lbl
FDA prescribing information — ORIAHNN (elagolix, estradiol, norethindrone acetate)
FDA prescribing information — NATAZIA (estradiol valerate / estradiol valerate and dienogest)
FDA-approved labeling — ESTRACE (estradiol tablets) 081295s014; EVAMIST (estradiol transdermal spray) 022014s015; ESTRACE (estradiol vaginal cream); estradiol vaginal inserts
FDA, Compounding and the FDA: Questions and Answers
Harlow SD et al. Abnormal uterine bleeding is associated with fatigue during the menopause transition. Menopause 2025;32(6):499–504 (SWAN, n=2,329)
Market and access
AMN Healthcare, 2025 Survey of Physician Appointment Wait Times — 41.8-day average new-patient OB/GYN wait across 15 large US metropolitan markets, fielded January–February 2025
Provider pages — read July 2026
Midi Health: pricing and insurance page; published clinical guidance on perimenopausal bleeding
Sesame: women’s health and service pages; menopause treatment page; terms of service
Winona: online menopause specialists page; hormone replacement therapy page
Inner Balance: Oestra product and perimenopause pages | Hers: menopause page
Last verified: July 2026