Some links on this page are affiliate links. We may earn a commission if you start care through them, at no extra cost to you. Affiliate relationships do not determine the evidence, the conclusions, or the order things appear in.
Start here: what the counter just told you
Find your line. Then read the section it points to.
| What you heard | What it usually means | Who fixes it | First question to ask |
|---|---|---|---|
| “It’s not covered” | The exact product isn’t on your plan’s list | Prescriber + plan | “Which estradiol patch is on my formulary?” |
| “It needs prior authorization” | It is covered — it’s gated | Prescriber | “What criteria do you need, and what’s been sent?” |
| “We can only give you 8” | A quantity limit, not an exclusion | Prescriber + plan | “What quantity and days supply were billed?” |
| “That’ll be $94” (it was $10) | Often a deductible reset — but not always | Depends | “Did the claim go through, or did it fail?” |
| “It’s backordered” | Supply, not coverage. No appeal fixes this | Pharmacist | “Can another manufacturer’s version be filled?” |
Not sure which one you’re in? The question in bold above is the one that separates half of these from the other half. It’s the most useful sentence on this page, and it’s free.
THIS PAGE IS FOR YOU IF
- The pharmacy quoted a price you didn’t expect
- You were told “not covered,” “needs approval,” or “refill too soon”
- Your copay jumped in January and nothing else changed
- You’re checking before your appointment so you’re not blindsided
- Your patch is backordered and you can’t tell if that’s an insurance problem
THIS PAGE IS NOT FOR YOU IF
- You want dosing help. Different question → Estradiol patch dosage guide
- You want vaginal estrogen coverage. Creams, rings, and tablets sit on their own formulary lines.
- You want a birth control patch. Xulane and Twirla are contraceptives — different rules entirely.
- You want gender-affirming hormone coverage. Real question, different rules.
- You’re outside the United States. Everything below is U.S. law and U.S. plans.
Does insurance cover estradiol patch?
Usually — but “covered” means your plan will pay for a patch, not necessarily your patch. Every commercial, Medicaid, and Medicare drug list we opened in 2026 lists at least one estradiol patch. None of them lists them all the same way. Which patch your plan picked, and what conditions it attached, is what decides your price.
There is a federal floor, and it’s real. Under 45 CFR § 156.122, a plan providing essential health benefits — non-grandfathered individual and small-group coverage, including Marketplace plans — must cover the greater of one drug in each category and class, or the same count as its state’s benchmark plan.
Read what that guarantees carefully. It’s a category-and-class floor. It does not guarantee a patch. Not the transdermal route, not your strength, not your schedule, and definitely not your copay. A plan could satisfy that rule with a pill.
The five documents we opened
We didn’t summarize other websites. We opened the payer documents and read them.
| Document | Date on it | What it shows | What it can’t tell you |
|---|---|---|---|
| Cigna — Drug Quantity Management policy, estrogen patches | Reviewed Jan 5, 2026 | Once-weekly patches capped at 4 per 28 days; twice-weekly at 8. Four written override paths. Combination patches capped with no override criteria published in this policy. | Whether any Cigna plan covers the drug. This is a quantity policy, not a formulary — your plan document controls. |
| Blue Cross and Blue Shield of Illinois — Performance Drug List | April 2026 | Both generic patches are non-preferred generics with a 30 per 30 days limit. The generic estradiol pill is a preferred generic. Climara Pro is marked as a preferred brand. | What a different BCBS plan does — including the second BCBS list right below this one. |
| Blue Cross and Blue Shield — Enhanced Drug List (bcbsil.com) | July 2026 | Same insurer. Same state. A differently structured list. | Your tier. It’s built differently and doesn’t print them the same way. |
| Montana Healthcare Programs (Medicaid) — Preferred Drug List | Revised Jan 15, 2026 | The generic once-weekly patch is preferred. The generic twice-weekly patches are not — but the brands Minivelle and Vivelle-Dot are. | What any of the other 49 states do. |
| Aetna Medicare FIDE (HMO D-SNP), Illinois — 2026 List of Covered Drugs | Formulary ID 26010, effective Jan 1, 2026 | A five-tier Part D ladder, 24- and 72-hour exception clocks, and a transition-fill rule most members never hear about. | Your Part D plan. There are hundreds, and each writes its own list. |
What this proves: the differences between plans are real, they’re written down, and they are not about your body.
What it doesn’t prove: national coverage rates, your copay, your tier, your plan’s accepted manufacturer, or what’s on the shelf today. Nobody can see your plan from the internet. What we can do is show you exactly what to look for and what it means when you find it.
What does “covered” mean for an estradiol patch?
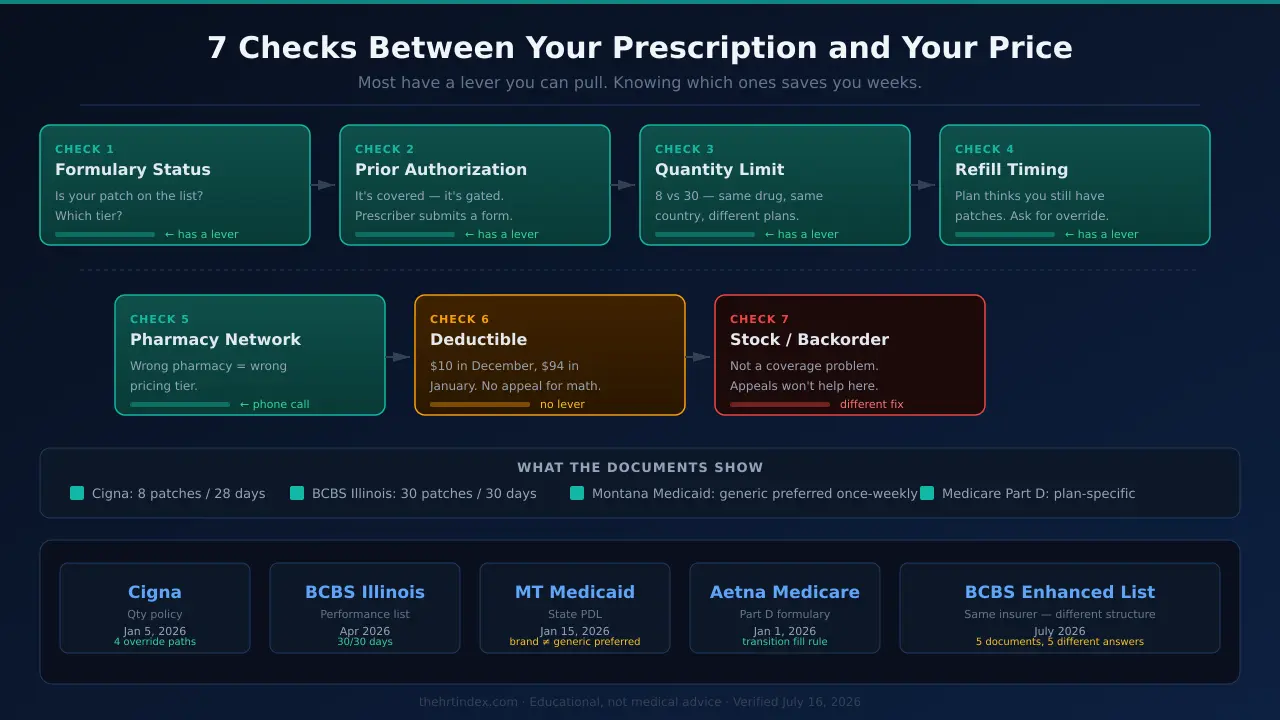
“Covered” means your plan lists the product and will pay something toward it under stated conditions. It does not mean cheap, and it does not mean the claim will process today. Seven separate checks sit between a prescription and a price, and they fail in different ways for different reasons.
- The exact product and its formulary status — is your patch on the list, and where?
- Prior authorization or step therapy — does someone have to justify it first?
- Quantity and days supply — how many will the plan pay for, in what window?
- Refill timing — does the plan think you still have patches left?
- Pharmacy network — is this pharmacy eligible for your best pricing?
- Deductible and cost sharing — what’s yours to pay before the plan pays?
- Stock — can the pharmacy physically get it?
Checks 1 through 4 usually have a written review or exception route. Check 5 is a phone call. Check 6, applied correctly, has no exception. Check 7 isn’t a coverage problem at all — and filing an appeal against it wastes a week you don’t have.
The vocabulary, in sixty seconds
| Term | What it means |
|---|---|
| Formulary | Your plan’s list of drugs it will pay for. Also called a drug list. Every plan has one. They’re all different. |
| Tier | Which price bucket your drug sits in. Tier numbers aren’t standardized — a “Tier 2” at one insurer is not a “Tier 2” at another. |
| Prior authorization (PA) | The drug is covered, but your plan wants your prescriber to justify it in writing first. |
| Step therapy (ST) | Your plan wants you to try its preferred option before it pays for yours. |
| Quantity limit (QL) | A cap on how many patches your plan will pay for in a set window. It’s a utilization rule, not proof the drug is excluded. It gets mistaken for a denial constantly. |
| NDC | National Drug Code — identifies the exact product and maker your pharmacy billed. Sometimes a claim fails on the code, not the drug. |
“Preferred” and “cheap” are not the same word
On Montana’s Medicaid list, “preferred” does one job: preferred products don’t go through the non-preferred prior-authorization route. Preferred goes through. Non-preferred needs a form first.
On Blue Cross of Illinois’ Performance list, “preferred” means something else entirely. That list runs six tiers — Preferred Generic, Non-Preferred Generic, Preferred Brand, Non-Preferred Brand, and two specialty tiers. So a “preferred brand” is the favored option among brands. It sits above a non-preferred generic on the ladder, not below it.
If you’re on Medicaid and your patch is non-preferred, your problem is a form, and it belongs to your prescriber. If you’re on a commercial tiered plan and your patch is a non-preferred generic, your problem is a copay, and the fix is a different conversation. Knowing which one you’re in tells you who to call.
The one with no lever: your deductible
Your deductible is what you pay yourself before your plan starts paying its share. It resets at the start of your plan year — often January 1, though not always.
This is the most common reason a patch costs $10 in December and $94 in January. Your coverage didn’t change. You’re paying the plan’s negotiated price yourself until you’ve met it again.
These are not small numbers. In KFF’s 2025 Employer Health Benefits Survey, among covered workers who faced a general annual deductible, the average single-coverage deductible was $1,886 — and 34% of covered workers were in a plan with a single-coverage deductible of $2,000 or more.
Your pharmacy said no. What does that actually mean?
A pharmacy rejection is a code, not a verdict. Different messages mean different things, and the review process attached to each one depends on what kind of plan you have. Get the exact rejection text before you do anything else.
| What the pharmacy says | What it usually means | The lever | Who’s next |
|---|---|---|---|
| “It’s not covered” / “not on your plan’s list” | The exact product isn’t on the formulary | Formulary exception | Prescriber statement, then the plan |
| “It needs prior authorization” | It is covered — it’s gated | PA submission — not an exception | Prescriber |
| “We can only give you 8” | Quantity limit — a utilization rule, not a category exclusion | Exception to waive the limit — CMS confirms a Part D exception can waive a utilization rule including a quantity limit | Prescriber + plan |
| “Refill too soon” | A timing edit — the plan thinks you still have patches | Ask for the earliest eligible date; if a mid-cycle switch caused it, ask what override applies | Pharmacy first |
| “Try the pill first” | Step therapy | Step-therapy exception | Prescriber |
| “Not at this pharmacy” | Network or channel rule | Ask which pharmacy or mail-order channel is preferred | You |
| “That’ll be $94” | Deductible, tier, or a claim that failed | Ask whether it adjudicated. That answer decides everything | Depends on the answer |
| “It’s on backorder” | Not a coverage problem. Every lever above is useless here | Different pharmacy, different manufacturer, or a documented switch | Pharmacist |
Which rulebook are you under?
This is the part most pages skip, and it’s why generic advice about deadlines gets women nowhere. The clock depends on your plan type.
| Your plan | The rule | The clock |
|---|---|---|
| Marketplace or small-group (essential health benefit plans) | 45 CFR § 156.122 | 72 hours standard for a non-formulary exception; 24 hours expedited when exigent circumstances apply |
| Medicare Part D / Medicare Advantage drug plan | CMS coverage determinations and exceptions | 72 hours standard, 24 hours expedited — starting when the plan receives your prescriber’s supporting statement |
| Large-group or self-funded employer plan | ERISA claims procedures | Use your denial notice and plan documents |
| Medicaid | Your state’s process | Use your state or managed-care plan’s criteria |
The 24-hour rule almost nobody knows about
45 CFR § 156.122(c)(2)(ii) defines “exigent circumstances” — the trigger that turns a plan’s 72-hour deadline into a 24-hour one. Exigent circumstances exist when your health may be seriously jeopardized or when you are already in the middle of a course of treatment using a drug that isn’t on the formulary.
If your plan is an essential health benefit plan, and you’re already on the patch, and your plan has dropped it from the formulary — being mid-treatment is written into the definition. You are not asking for a favor. You are describing a condition the regulation already names.
The words that matter: “I’m requesting an expedited non-formulary exception.” Then ask them to confirm the time they received it.
Important scoping notes:A tier change is not automatically the same thing. If your patch is still on the list but moved to a worse tier, that’s a different request, and the 24-hour exigent trigger doesn’t automatically attach. And this rule doesn’t govern every plan — it covers non-grandfathered individual and small-group coverage.
What your prescriber actually has to say
For a Part D tiering exception, CMS is specific: your prescriber’s statement has to say the preferred drug wouldn’t be as effective for you.
When nothing happens for six days, make two calls. Ask the prescriber’s office for the submission date. Ask the plan for the receipt date, the case number, and the request type.Whichever one can’t answer is your answer.
You know which lever moves your patch. The next question is who’ll pull it.
The right online HRT provider isn’t the same for every woman — it depends on your symptoms, your age and whether you have a uterus, your medication route preference, your risk history, your insurance or cash-pay situation, and your state. Use The HRT Index’s Find My HRT Path tool to match your situation to the right provider — and to flag when online care isn’t the right starting point.
Get my personalized action plan →Free · About 90 seconds · No email required to start
Which estradiol patch does your plan actually cover?
Most estradiol patches have an FDA-approved generic — which is why the drug is cheap. But “generic” is an approval status, not a coverage status, and not a promise the product is on a shelf.Approval, marketing, and formulary placement are three different systems that don’t check with each other.
| Reference brand | Schedule | Strengths (mg/24h) | FDA generic? | Marketed now? | How our lists treat it |
|---|---|---|---|---|---|
| Vivelle-Dot (Noven) | Twice weekly | 0.025–0.1 | Yes — incl. Dotti | Yes | BCBSIL: generic non-preferred, QL 30/30 days. Montana: brand preferred, generic non-preferred. Ships 8 per box. |
| Minivelle (Noven) | Twice weekly | 0.025–0.1 | Yes — incl. Lyllana | Yes | Montana: brand preferred; Lyllana non-preferred. Ships 8 per box. |
| Climara (Bayer) | Once weekly | 0.025–0.1 (incl. 0.06) | Yes | Yes — not discontinued | BCBSIL: generic non-preferred, QL 30/30. Montana: generic preferred, brand non-preferred. Ships 4 per box. |
| Menostar (Bayer) | Once weekly | 0.014 | Yes — FDA approved Zydus generic Apr 17, 2023 | Apparently not commercially available (Drugs.com, Jun 11, 2026) | BCBSIL: brand only, non-preferred, QL 30/30. Montana: non-preferred. Sole approved use: bone loss prevention — not hot flashes. |
| Alora | Twice weekly | 0.025–0.1 | No | No — Discontinued March 2021 | BCBSIL still lists it as a covered brand with a 2026 quantity limit. Yes, really. See the supply section. |
Look at the Menostar row for a second, because it’s the whole page in one line. A generic exists on paper. It doesn’t appear to exist in a pharmacy. And the drug list shows only the brand. Three systems, three answers, one drug.
Why “ask for the generic” can still fail
It’s the most common advice about this drug, and it’s a coin flip. Here’s Montana Medicaid’s transdermal section, revised January 15, 2026, exactly as the columns read:
| Schedule | Preferred (no non-preferred PA route) | Non-preferred (prescriber files first) |
|---|---|---|
| Once-weekly | Generic estradiol patch (for Climara) | Climara (the brand) |
| Twice-weekly | Minivelle and Vivelle-Dot (the brands) | Generic twice-weekly patches · Dotti · Lyllana |
| Gels and spray | — | Divigel, Elestrin, generic gel packet, gel pump, Evamist |
| Also non-preferred | — | Menostar |
A woman in Montana who’s told “just ask for the generic” and hands over a twice-weekly prescription gets stopped at the counter. A woman told “always ask for the brand” and handed a once-weekly prescription gets stopped too. The advice inverts depending on which patch you wear — and nothing about that is medical.
The two brand-name patches this plan actually covers
The Blue Cross of Illinois Performance list is a closed list — its own introduction says every covered drug is shown. Which leaves exactly two estradiol-only patch brands printed as covered entries on that list:
- ALORA — non-preferred, with a 2026 quantity limit. Discontinued since 2021.
- MENOSTAR — non-preferred, with a quantity limit. The only estrogen patch whose sole approved use is preventing bone loss.
One hasn’t been manufactured in five years. The other isn’t approved for hot flashes.
The Menostar trap
Menostar’s only approved use is preventing bone loss after menopause. If Menostar gets prescribed for hot flashes, that’s off-label — and a plan can deny it on the indication alone. That’s not a formulary problem. It’s an indication mismatch, and it’s a different conversation.
Two corrections to things circulating right now
1. “Bayer discontinued Climara.”No. Cigna’s national policy — reviewed January 5, 2026 — still lists Climara with active override criteria, and Montana’s January 2026 list still carries both the brand and its generic. Climara is not discontinued.
2. “Alora was discontinued in the 2026 shortage.” No. FDA’s drug shortage database recorded the discontinuation in March 2021. Cigna pulled it from its patch policy as obsolete in the January 2025review. It’s a five-year-old exit being recycled as breaking news.
If we’ve got either wrong, email corrections@thehrtindex.comand we’ll log it with the date and the change.
Does having a uterus change which patch you should search for?
It can — and if it does, you may be searching your formulary for the wrong word. FDA labeling states that when systemic estrogen is prescribed to a postmenopausal woman with a uterus, adding a progestogen has been shown to reduce the risk of endometrial hyperplasia and endometrial cancer. That progestogen can come separately, or built into a combination patch. A combination patch is a different drug with its own formulary line and its own rules.
The two combination patches: CombiPatch (estradiol + norethindrone acetate, twice weekly) and Climara Pro (estradiol + levonorgestrel, once weekly). Neither one is an “estradiol patch” on a drug list. If your prescription says CombiPatch and you searched your portal for estradiol, you searched the wrong word and got the wrong answer.
| Patch | BCBS Illinois Performance list (Apr 2026) | Cigna quantity policy (Jan 5, 2026) |
|---|---|---|
| Climara Pro | Preferred brand (P) — no quantity limit shown | Quantity limit applies, but no override criteria published in this policy |
| CombiPatch | Non-preferred (NP) — no quantity limit shown | Same — quantity limit without published override criteria |
| Any estradiol-only generic patch | Non-preferred generic — 30/30 quantity limit | Override criteria published (strength change, two-patch, fertility, gender-affirming) |
What to do if you have a uterus and are prescribed a patch:
- Search your formulary for the exact product on your prescription — CombiPatch or Climara Pro, not “estradiol.”
- Search the generic description too — “estradiol/norethindrone” or “estradiol/levonorgestrel.”
- If you get a quantity rejection on a combination patch, don’t assume the standard override language applies. Ask your plan: “What is the exception process for this specific product?”
- Don’t switch products to chase coverage. Combination patches deliver two hormones for a reason. Coverage is a reason to file paperwork, not to change medicine.
Why will my plan only cover 8 patches a month?
Because of a quantity limit — a cap on how many patches your plan will pay for in a set window.It’s a utilization rule, not proof the drug is excluded, and it reads like a denial when it isn’t one. How many you get has nothing to do with your body.
| | Cigna quantity policy (Jan 5, 2026) | BCBS Illinois Performance list (Apr 2026) |
|---|---|---|
| Once-weekly patch (Climara type) | 4 per 28 days retail · 12 per 84 days home delivery | 30 per 30 days |
| Twice-weekly patch (Vivelle-Dot type) | 8 per 28 days retail · 24 per 84 days home delivery | 30 per 30 days |
The limits match the box
Cigna’s policy lists package sizes right next to the limits. Climara ships 4 patches per box. The once-weekly limit is 4 per 28 days. Vivelle-Dot and Minivelle ship 8 patches per box. The twice-weekly limit is 8 per 28 days.
The numbers match the carton counts exactly.The policy doesn’t say packaging is the reason. But once you’ve seen it, the limit stops looking like a judgment about your dose and starts looking like a unit of inventory.
A twice-weekly patch means about 8 or 9 patches a month. The cap is 8. The limit sits exactly on your dose, with no headroom at all.So anything that moves — a strength change mid-cycle, a pharmacy substitution, a refill a few days early — can push the billed quantity past a 28-day window and reject the claim.
The override paths — written down, and almost never mentioned
Cigna’s policy spells out when it will approve more. This is the fine print that turns a dead end into a request your prescriber can make in one sentence.
| Your situation | What Cigna’s policy allows |
|---|---|
| Changing strengths (within same schedule) | A one-time override: 4 extra patches (once-weekly) or 8 extra (twice-weekly) at retail — approvable once every 30 days |
| On 0.075 or 0.1 mg and needing two patches at once | 8 per 28 days for once-weekly; 16 per 28 days for twice-weekly |
| IVF or fertility protocols (if infertility is a covered benefit) | The requested quantity |
| Gender-affirming care (0.1 mg twice weekly) | Up to 32 patches per 28 days |
Approvals generally run one year. One-time overrides run 30 days. This is Cigna’s policy — illustrative, not universal. Walk into your plan knowing these numbers exist somewhere, and ask where yours are.
The catch that also cuts your way
Straight out of the Blue Cross drug list: a dispensing limit doesn’t stop you from getting more patches. It stops your plan from paying for the extras. If you need two extra patches to reach your next refill date and an appeal would take 72 hours, ask the pharmacist what the extras cost in cash for your exact product and strength. Sometimes that answer solves your week.
If your plan pushes you to a 90-day fill
Many plans cover up to a 90-day supply of maintenance medications, and hormone therapy qualifies. But look at Cigna’s home-delivery column: 12 patches per 84 days for once-weekly; 24 per 84 days for twice-weekly.
Eighty-four days, not ninety. Plans often use “90-day” as the name of the benefit while the claim itself gets billed for 84 days on a product packaged in 28-day cycles. Before you move to mail order, ask: “What quantity and how many days’ supply will actually be billed?” Get the number. Not the word.
How do I check my exact estradiol patch coverage before I pay?
Your member formulary is the only source that can answer this, and you can usually reach it in about ten minutes.Look up the exact product and schedule on your own plan’s drug list, record the tier and every restriction, then ask for a member-specific price before you hand over a card.
- Find out who actually runs your drug benefit. Your medical insurer and your pharmacy benefit manager are often different companies. Look at your card: if there’s a separate Rx number, an “Rx BIN,” or a different logo near the prescription section, that’s who decides this.
- Open your member-specific drug list. In priority order: your logged-in member portal, then your plan’s exact Summary of Benefits or formulary document. A public PDF you found online is a preliminary reference — useful, but it may not be your benefit design.
- Search the generic description and the exact product name. Search “estradiol transdermal,” “estradiol patch,” and the brand written on your prescription. If it’s a combination patch, search CombiPatch or Climara Pro by name.
- Match the schedule and strength. Once-weekly and twice-weekly are separate entries. This is the single most common place people get a right answer to the wrong question.
- Write down every restriction. Not just “covered.” The worksheet below has every field.
- Ask for the member-specific price, then get a reference number. Say: “Please price this exact estradiol transdermal product, strength, quantity, and days supply at this pharmacy. Is that price a copay, coinsurance, or a deductible?” Then get the representative’s name and a reference number. Every time.
The exact fields to write down before you call
Product name (exactly as written): Generic or brand: Strength (mg/24hr): Once-weekly or twice-weekly: Combination patch? (CombiPatch / Climara Pro): Quantity billed: Days supply billed: Manufacturer / NDC: Pharmacy (and is it in network?): Rejection code and exact wording: Did the claim adjudicate, or fail? Formulary status / tier: PA / step therapy / quantity limit? 30-day or 90-day requirement: Member price quoted: Plan type (Marketplace / small group / large group / self-funded / Part D / Medicaid): Rep name + reference number: Date checked:
The last two lines are the ones people skip and regret. Get the reference number. Every time.
Who can prescribe this so your insurance actually pays?
Two separate benefits decide your cost. Your medical benefit pays for the visit. Your pharmacy benefitpays for the patch. They’re independent — which means you don’t need your visit covered for your patch to be covered.
| | Midi Health | Sesame | Winona |
|---|---|---|---|
| Visit billed to insurance? | Yes — in-network with most PPO plans (Midi’s statement) | No — cash-pay | No — cash-pay |
| Prescription sent to your pharmacy? | Yes | Yes | No — ships to you |
| Can your drug benefit pay for the patch? | Yes | Yes | No — no claim submitted |
| Medicare | Not billed or accepted — self-pay possible, no claims | Cash-pay visit — your Part D still works at the pharmacy | No |
| Medicaid | Not at all, even self-pay | Check eligibility directly | No |
| Current price | Varies by plan — that’s the point | Menopause treatment from $54/mo (checked 07/16/2026) | Estrogen patch from $149/mo (checked 07/16/2026) |
If you have PPO insurance and you want it billed
Midi Health states it is in-network with most PPO plans, that coverage varies, and that deductibles, coinsurance, and copays may still apply. It’s available in all 50 states and prescribes FDA-approved hormone therapy — including patches — to your own pharmacy, which is what lets your drug benefit pay for anything.
Three things to know before booking Midi:
1. Medicare: not billed, not accepted.Midi states it is not covered by Medicare or any Medicare-related plan. Medicare beneficiaries can be seen as self-pay — but Midi states they cannot submit claims to Medicare for visits, medications, or related services.
2. Medicaid: closed entirely. Midi states it is not enrolled and not participating with state healthcare programs including Medicaid and Medi-Cal, and cannot treat Medicaid patients — even as self-pay.
3. It has a public complaint record. As of July 16, 2026, Midi holds a B rating from the Better Business Bureau, with 154 complaintsfiled in the BBB’s three-year reporting window. A count is not a rate — BBB doesn’t publish how many patients Midi has seen.
Midi does not ship you a prepackaged box of hormones. If a flat monthly price with zero billing surprises is your priority, a direct-ship service is better for you. But because Midi skips the box, it can send an FDA-approved patch to your pharmacy on yourinsurance. That’s the trade.
The surprise is preventable. Before you book:
- Call the number on your card. Ask: “Is Midi Health in-network for a telehealth visit under my plan?”
- Ask: “Have I met my deductible this year? What’s my specialist copay or coinsurance?”
- Ask: “Is [your patch, by name and strength] on my formulary? What tier? Is there a quantity limit or a prior authorization?”
- Write down the reference number and the rep’s name.
You have a PPO, you’re not on Medicaid, and you want your patch running through your own pharmacy on your own benefit.
That’s the exact case Midi is built for. Check availability for your state and insurance carrier.
Check Midi’s coverage for your state →Affiliate link. We may earn a commission. Nothing above changes because of it — every claim is dated and sourced.
If your visit isn’t the part you need insured
Sesame states that all visits are cash-pay and it does not accept insurance — but that if you have insurance and get a prescription during your appointment, your prescription may still be covered depending on your plan, and the pharmacist can check your coverage at pickup. Prescriptions go to your preferred pharmacy. As of July 16, 2026, Sesame advertises menopause treatment from $54 per month, with medication priced separately. Visits are HSA/FSA-eligible.
And this is the door for Medicare. If Midi is closed to you because it won’t bill Medicare, a cash-pay visit that sends an FDA-approved patch prescription to your own pharmacy lets your Part D benefitdo exactly what it exists to do. Nobody tells Medicare beneficiaries this, and it’s the cleanest route on this page for them.
Midi isn’t in your network — or your deductible makes “covered” meaningless — or you’re on Medicare.
Paying cash for the visit and letting your drug benefit cover the patch is a real path — and it’s the one most people miss. See Sesame’s current menopause-care price.
See Sesame’s current menopause-care price →Affiliate link. We may earn a commission. Sesame does not bill insurance for the visit — verify your patch’s pharmacy coverage separately.
Who this section is not for
- Medicaid: the platforms above don’t serve you. Your path is your own prescriber plus your plan’s criteria. See HRT insurance coverage.
- You want a compounded cream: compounded hormone products are not FDA-approved, and reimbursement is plan-specific and often limited. → FDA-approved vs. compounded HRT
- A history of breast cancer, thromboembolic disease, or unexplained genital bleeding: this needs clinician review. Use in-person or specialist care when the evaluating clinician directs it.
Does Medicare cover the estradiol patch?
Some Part D and Medicare Advantage drug plans list one or more estradiol patches, but coverage is plan-specific because each plan writes its own formulary. A retail, self-administered patch runs through Part D or a Medicare Advantage drug benefit rather than Part B. In 2026, no Part D plan can charge more than a $615 deductible, and once you’ve spent $2,100 out of pocket on covered Part D drugs, you owe $0 for covered drugs the rest of the calendar year.
Four things nobody tells Medicare enrollees about this drug:
We opened a real 2026 Medicare drug list — the Aetna Medicare FIDE (HMO D-SNP) formulary for Illinois, formulary ID 26010, effective January 1, 2026 — and it spells out a transition rule that most members never hear at a counter.
For a new member, that plan will cover a temporary 30-day supply during the first 90 days if: the drug isn’t on the plan’s list, or the plan’s rules won’t let you get the amount your prescriber ordered, or the drug needs prior authorization, or the drug is caught in a step-therapy rule.
The move isn’t to quote Aetna. The move is to say the words at the counter: “I’m a new member — can this run as a transition fill?” Use the month to file the exception.
On routing: Midi won’t bill Medicare. But a cash-pay visit that sends a prescription to your own pharmacy leaves your Part D benefit fully intact. → HRT insurance coverage
The Medicare Prescription Payment Planspreads your covered out-of-pocket costs across the calendar year instead of hitting you all at once in January. It doesn’t reduce what you owe — it changes when you owe it.
Does Medicaid cover the estradiol patch?
Medicaid coverage is state- and plan-specific, and the first thing to find out is which drug list controls yours.Your pharmacy benefit runs either through fee-for-service Medicaid or through a managed-care plan, and states differ on which one sets the rules. Then check that list for your exact product and schedule — because the answer can turn on something as small as whether you wear it once a week or twice.
Montana’s list, revised January 15, 2026:
- Preferred: the generic once-weekly estradiol patch. Plus the brands Minivelle and Vivelle-Dot.
- Non-preferred: the generic twice-weekly patches, Dotti, Lyllana, brand Climara, Menostar — plus every estradiol gel and the spray.
Note the gels and spray: in Montana, if a supply problem pushes you off your patch onto a gel, the gel is non-preferred too. The escape hatch has a lock on it.
One bright spot worth naming: Illinois’ HB 5295, effective January 1, 2026, extends menopause therapy coverage to Medicaid in certain circumstances.
- Find out whether your pharmacy benefit runs through the state or your managed-care plan. That determines which list controls.
- Search that list for “estradiol” and check which column it’s in, by schedule.
- If it’s non-preferred, get the exact criteria. Don’t guess what your state wants documented. Ask for the prior-authorization criteria for that specific product, then hand them to your prescriber.
And again: the telehealth platforms on this page don’t serve Medicaid patients. Midi cannot treat Medicaid patients even if you offer to pay cash. → HRT insurance coverage guide
Your patch is covered, but the pharmacy doesn’t have any. Now what?
This is a supply problem, not a coverage problem — and every appeal on this page is the wrong tool for it.ASHP’s drug shortage bulletin lists estradiol transdermal systems as a current shortage, with availability differing by manufacturer. Your patch can be unavailable at one pharmacy and sitting on a shelf three miles away. There is no form that fixes that.
| | Coverage problem | Supply problem |
|---|---|---|
| What you hear | “Not covered” · “needs approval” · “refill too soon” · a price | “Backordered” · “we’re out” · “check back tomorrow” |
| The fix | Exception, PA, or quantity override | Different pharmacy · different manufacturer · documented switch |
| Who fixes it | Prescriber + plan | Pharmacist + prescriber |
| The clock | 24 or 72 hours, depending on plan type | None |
| Does an appeal help? | Yes | No. Zero. Wrong tool entirely. |
The document that proves the whole point
Alora is gone. Permanently discontinued — not in shortage, not backordered, not coming back. FDA’s drug shortage database recorded the discontinuation in March 2021. Cigna pulled it from its patch policy as obsolete in the January 2025 review.
And Blue Cross and Blue Shield of Illinois’ Performance Drug List, dated April 2026 — a live, current, tiered formulary — lists ALORA as a covered non-preferred brand with a quantity limit of 30 patches per 30 days.
When a supply fix creates a coverage rejection
During a shortage, your pharmacy substitutes what it can get. Say you’re on a twice-weekly generic and the only thing in stock is a once-weekly generic. Your prescriber approves it.
Remember what Cigna’s policy said? The quantity limit accumulates across weekly and twice-weekly patches combined.So the patches you already picked up this month count against the ones you’re picking up now. The claim rejects. The pharmacist says “refill too soon.” And you go home thinking your insurance dropped your medication.
Say it that way.Don’t call it a strength change — Cigna’s strength-change override is written for changing strengths within the same schedule, and a stock-driven switch to a different schedule isn’t that. Describe what actually happened and let them route it.
What to ask your pharmacist
Those are completely different problems and they look identical from your side of the glass. A claim that processed and left you with $94 is a deductible or a tier. A claim that failed is a formulary, quantity, or timing issue. One has a lever. The other doesn’t. You cannot tell which one you’re in until you ask.
Then, if it’s stock:
- “Can another manufacturer’s version be filled instead?” Availability is manufacturer-by-manufacturer right now, not drug-wide.
- “Which NDC are you billing?” Sometimes a claim fails on the code, not the drug.
- “Can you check inventory at other locations in your chain?” Many can.
- “Can we transfer the prescription?” Confirm the other pharmacy is in-network first.
- “What about mail order?” Larger fulfillment centers sometimes have stock when retail doesn’t.
- “Does this change need a new prescription?” Ask — it depends on the product, the prescription, and your state’s substitution rules.
One real, named, on-the-record account. Not medical evidence. Not a claim her experience is typical. We have no relationship with her.
Supply status changes constantly. Check ASHP’s current bulletin and FDA’s shortage database yourself before you act on any snapshot — including ours.
You’ve called four pharmacies. Three different people have told you no.
If your plan won’t cover it, your deductible makes “covered” meaningless, or you simply cannot find one — a flat published cash price shipped to you is a legitimate answer. Winona states it does not work directly with insurance companies and cannot bill your insurance, though it can provide documentation and HSA/FSA receipts may be reimbursable. As of July 16, 2026 it advertises an estrogen patch from $149 per month, shipped — alongside compounded creams, which are a different regulatory category entirely.
Two things to be straight about before you click: Winona won’t submit a claim for you, so your plan sees nothing. And confirm you’re getting the FDA-approved patch, not a compounded cream, before you pay.Winona states its patch is FDA-approved; we haven’t independently confirmed the dispensed product, so check what’s in your cart.
See Winona’s current patch price and treatment details →Affiliate link. We may earn a commission. Verify the current price at checkout.
Does your state’s menopause law actually help you?
Only if the law covers your product and your plan type — and for most people, it won’t reach the plan. State insurance law generally doesn’t bind private self-funded employer plans, which are governed by federal ERISA rules instead. KFF reports 67% of workers covered through an employer health plan were in a self-funded plan in 2025, and 80% at firms with 200 or more employees.
| State | Where it stands |
|---|---|
| Illinois | HB 5295, effective Jan 1, 2026, requires coverage of medically necessary hormonal and non-hormonal menopause therapy for group and individual policies, managed care, and Medicaid in certain circumstances — including all FDA-approved forms: oral, transdermal, topical, and vaginal rings. HB 5492, signed June 28, 2026, requires coverage of six months of HRT and supplies — effective 2028. |
| Louisiana | Mandate effective Aug 1, 2024; includes hormone therapy |
| New Jersey | Menopause Coverage Act — carriers must cover medically necessary perimenopause and menopause treatment, including hormonal therapies |
| Maryland | SB 892 / HB 1365 — provider-training provisions effective July 1, 2026; insurance coverage provisions don’t start until Jan 1, 2027, and only for policies issued or renewed on or after that date |
Several other states have acted on menopause care in narrower ways. If your state isn’t above, look up the enacted bill, its effective date, and which plan types it reaches before you count on it.
Why the headline you read probably doesn’t apply to you
Maryland passed a menopause insurance law. By its own legislature’s math, the plans it can regulate cover fewer than one in five Marylanders under 65.
The proof is sitting on your own drug list
Open the Blue Cross of Illinois Performance Drug List from April 2026 and read two sections about forty lines apart.
In the contraceptives section: the generic contraceptive patch and Twirla both carry an “AC” flag — the list’s mark for Affordable Care Act preventive coverage. Products marked that way may have limited or $0 member cost-sharing.
In the estrogens section, on the same list: the generic estradiol patch is a non-preferred generic with a quantity limit. No AC flag. No $0 pathway. No copay-waiver process. Just a tier and a cap.
One question to HR settles which world you’re in: “Is our health plan fully insured or self-funded?”It takes them three seconds, and it changes which rules you’re playing under.
Is the estradiol patch cheaper without insurance?
Sometimes — especially early in the plan year, or on a high-deductible plan. A cash or discount price on a generic patch can come in under a copay, and it can beat paying a negotiated price against an unmet deductible.
- 8 generic 0.025 mg/24hr twice-weekly estradiol systems from $35.83
- 4 generic 0.025 mg/24hr once-weekly estradiol systems from $54.57
Read those together. The twice-weekly 8-pack costs lessthan the once-weekly 4-pack. Roughly a month of therapy either way — but if your plan is pushing you toward one schedule and your wallet is pushing toward the other, that’s worth knowing before you decide.
Three things before you reach for the coupon:
1. You can’t stack a discount card with insurance. One or the other, per fill.
2. Cash spending can be invisible to your plan. A discount-card purchase generally isn’t credited automatically to a commercial deductible or out-of-pocket limit. And a purchase made outside the Part D benefit doesn’t automatically count toward Part D true out-of-pocket spending. If you’re on track to hit your deductible or your cap anyway, saving $40 in February can cost you more in October.
3. Ask them to compare both ways.Ask whether the pharmacy can price the insurance claim against its cash or discount route for the same exact fill. Most women don’t know to ask. It’s the easiest money on this page.
Did FDA’s 2025–2026 label changes affect coverage?
Nothing in the plan documents we opened shows the label action changing the patch restrictions they display. Labeling and coverage are separate systems, run by different people, on different timelines. What the change did do is drive a surge in demand that made patches harder to find.
| Document | Date | Where it falls relative to FDA action |
|---|---|---|
| FDA class-wide label change announcement | November 10, 2025 | The announcement — not a switch being flipped |
| First six updated product labels approved | February 12, 2026 | Not one of them is an estradiol patch |
| Cigna quantity policy | Jan 5, 2026 | After announcement, before first approvals |
| Montana Medicaid PDL | Jan 15, 2026 | After announcement, before first approvals |
| BCBSIL Performance list | April 2026 | After both |
| BCBSIL Enhanced list | July 2026 | After both |
Labels moved. These formularies didn’t.
Four documents can’t prove no U.S. formulary changed, and they can’t prove causation in either direction. What they show is that the restrictions women are hitting right now were re-published after the news that supposedly fixed everything. If you’ve been wondering why the headlines and your pharmacy counter disagree — that’s why.
Nothing on this page says hormone therapy is right for you. A formulary tells you what your plan will pay for. Tier placement is an accounting decision, not a medical opinion — a preferred drug isn’t safer, and a non-preferred one isn’t worse for you. Those two systems have nothing to do with each other.
What we actually verified
We opened and read the primary documents behind the coverage and policy claims on this page. Not summaries of them. The documents.
| What we verified | Source | Evidence type | Date |
|---|---|---|---|
| Patch quantity limits (4 and 8 per 28 days retail; 12 and 24 per 84 days home delivery), package sizes, four override paths, approval durations, combination patch exclusion from override criteria | Cigna National Formulary Coverage Policy — Estrogens (Topical), Patches, Drug Quantity Management | Primary (payer policy) | Reviewed 01/05/2026 |
| Alora removed from Cigna policy as obsolete | Cigna policy revision history | Primary | 01/29/2025 |
| Generic patches non-preferred with QL 30/30; generic pill preferred; Climara Pro preferred brand; Alora and Menostar brand entries; ACA-preventive flag on contraceptive patches; dispensing-limit and exception language | Blue Cross and Blue Shield of Illinois Performance Drug List | Primary (formulary) | April 2026 |
| A second, differently structured drug list from the same insurer | Blue Cross and Blue Shield Enhanced Drug List (bcbsil.com) | Primary | July 2026 |
| Generic once-weekly patch preferred; Minivelle and Vivelle-Dot preferred; generic twice-weekly patches, Dotti, Lyllana, Climara, Menostar non-preferred; gels and spray non-preferred; brand-over-generic-preferences section | Montana Healthcare Programs Preferred Drug List | Primary (state PDL) | Revised 01/15/2026 |
| 2026 Part D tier ladder; 24/72-hour exception clocks; 30-day transition-fill rule covering non-formulary drugs, quantity limits, PA, and step therapy | Aetna Medicare FIDE (HMO D-SNP) 2026 List of Covered Drugs, Illinois — Formulary ID 26010 | Primary (Medicare formulary) | Updated 10/01/2025, effective 01/01/2026 |
| EHB category-and-class floor, formulary exception rights, timeframes, exigent-circumstances definition, external review | 45 CFR § 156.122, eCFR | Primary (federal regulation) | Current as of 06/17/2026 |
| Part D exception and coverage determination timeframes; exceptions can waive utilization management | CMS — Coverage Determinations and Exceptions | Primary | Retrieved 07/16/2026 |
| 2026 Part D deductible cap ($615) and out-of-pocket threshold ($2,100) | medicare.gov | Primary | Retrieved 07/16/2026 |
| Self-funded enrollment (67%; 80% at large firms); average deductible ($1,886); 34% at $2,000+ | KFF 2025 Employer Health Benefits Survey | Primary (survey) | Published 10/2025 |
| Share of Maryland under-65 residents in state-regulated commercial coverage (17.4%) | Maryland Dept. of Legislative Services fiscal note | Primary | 2026 session |
| No federal menopause-treatment coverage mandate | Maryland Health Care Commission analysis | Primary | 12/2025 |
| FDA generic approval for Menostar (Zydus, 04/17/2023); apparent lack of commercial availability | FDA / Zydus approval record; Drugs.com availability page | Primary + secondary | 04/2023; 06/11/2026 |
| Alora discontinued — all formulations | FDA drug shortage database; Drugs.com availability page | Primary + secondary | 03/2021; 06/11/2026 |
| Estradiol transdermal systems listed as a current shortage | ASHP Drug Shortage Bulletin (Univ. of Utah Drug Information Service) | Secondary | Updated 07/01/2026 |
| FDA label-change announcement and first six approved labels | FDA announcements | Primary | 11/10/2025; 02/12/2026 |
| Cash prices for two exact fills | Drugs.com price guide | Secondary | Retrieved 07/16/2026 |
| Midi Health’s Medicare and Medicaid statements, PPO language, state availability, BBB rating (B) and complaint count (154) | joinmidi.com; Better Business Bureau | Provider-stated; secondary | Retrieved 07/16/2026 |
| Sesame’s cash-pay model and current menopause price | sesamecare.com | Provider-stated | Retrieved 07/16/2026 |
| Winona’s insurance language, patch price, and FDA-approved claim | bywinona.com | Provider-stated — dispensed product/NDC not independently verified | Retrieved 07/16/2026 |
| One named account of a supply problem | NPR | Secondary (reporting) | 03/2026 |
What we did not do. We did not test any provider. We did not verify your specific plan. We did not audit an individual pharmacy claim. We did not call all fifty state Medicaid programs. We did not calculate a national coverage rate, because our sample can’t support one. We did not have a clinician review this page, and we’re not going to tell you we did.
What could be out of date. Formularies change mid-year. Supply changes weekly. Prices change. Every number here carries the date we saw it. If one’s wrong, tell us: corrections@thehrtindex.com — material corrections get logged with the date and the change.
How we work. This page was produced under The HRT Index Verification Standard — we read every published price or coverage term ourselves, separate FDA-approved from compounded, verify state availability and insurance, and re-check on a fixed schedule.
Frequently asked questions
Does insurance cover the estradiol patch?
Usually — every commercial, Medicaid, and Medicare drug list we opened in 2026 lists at least one estradiol patch. But your plan covers specific entries, not the category. Marketplace and small-group plans must cover at least one drug per category and class, and estrogens are a category — though that floor doesn’t guarantee a patch, a strength, a schedule, or a price.
How much is the estradiol patch with insurance?
There’s no reliable national number, because your cost depends on your tier, deductible, copay or coinsurance, quantity, pharmacy, and fill length. For a reference point: on July 16, 2026, Drugs.com listed 8 generic twice-weekly 0.025 mg/24hr systems from $35.83. If your copay is higher than a cash price, that’s usually your deductible — but ask whether the claim adjudicated before you assume.
Why is my estradiol patch not covered?
It’s usually one of seven things: your plan prefers a different patch, you hit a quantity limit, it needs prior authorization or step therapy, the refill was too soon, the pharmacy isn’t in network, your deductible reset, or the pharmacy can’t get it. Only some of those are “not covered” in the way you’re thinking. Get the exact rejection code — it tells you which one.
Is Vivelle-Dot covered by insurance?
It depends on the list, and the answer can be counterintuitive. On Blue Cross of Illinois’ April 2026 Performance list, the generic twice-weekly patch is a non-preferred generic with a 30-per-30-days limit, and the brand appears only as a reference brand. On Montana’s Medicaid list, the brand Vivelle-Dot is preferred while the generic twice-weekly patches are not. Search both the brand and the generic in your own plan’s portal.
Does insurance cover CombiPatch or Climara Pro?
They’re separate drugs with their own formulary lines, so searching “estradiol patch” won’t find them. Coverage can be better or worse than the single-hormone patch: on Blue Cross of Illinois’ April 2026 Performance list, Climara Pro is marked as a preferred brand while every estradiol-only patch is non-preferred. But Cigna’s national quantity policy notes that combination patches carry quantity limits without publishing override criteria for them. Search the exact product name.
Does Medicare cover the estradiol patch?
Some Part D and Medicare Advantage drug plans list one or more estradiol patches, but each plan writes its own formulary. A retail self-administered patch runs through Part D rather than Part B. Estrogens are not one of Medicare’s six protected classes, so your plan has real discretion. In 2026, no Part D deductible exceeds $615, and after $2,100 out of pocket on covered Part D drugs you owe $0 for the rest of the year.
I just switched Medicare plans and my patch stopped working. What now?
Ask the pharmacy to run it as a transition fill. Part D plans provide temporary transition supplies for new members under a CMS framework, and the 2026 Aetna D-SNP formulary we opened applies its 30-day transition supply not just to drugs missing from the list, but also to drugs blocked by a quantity limit, a prior authorization, or step therapy. Terms vary by plan — ask yours whether your rejected claim qualifies.
Does Medicaid cover the estradiol patch?
Usually, but it’s state- and plan-specific. First find out whether your pharmacy benefit runs through fee-for-service Medicaid or a managed-care plan, then check the controlling list. In Montana, the once-weekly generic is preferred while the twice-weekly generics aren’t — and the twice-weekly brands are. Some states require managed-care plans to follow a single statewide list; don’t assume yours does.
Why will my insurance only cover 8 patches a month?
That’s a quantity limit, and it’s a plan-by-plan number, not a medical one. Cigna’s national policy displays 8 per 28 days for twice-weekly patches; Blue Cross of Illinois displays 30 per 30 days for the same product. Notably, 8 is also exactly what fits in one manufacturer’s box. It reads like a denial but it’s a utilization rule — your prescriber can request an override, and documented criteria exist.
What is a formulary exception and how long does my plan have to answer?
It’s a request asking your plan to cover a drug that isn’t on its list, or to waive a rule like a quantity limit. For Marketplace and small-group plans, federal rules give the plan 72 hours standard and 24 hours for an expedited non-formulary request when exigent circumstances apply — and being mid-treatment on a non-formulary drug is written into that definition. Other plan types run their own processes.
My patch needs prior authorization. How long does that take?
It varies by plan. On Medicare Part D, an exception request gets 24 hours expedited or 72 hours standard — but that clock doesn’t start until the plan receives your prescriber’s supporting statement, and a routine prior-authorization determination can run on different timing. Ask the plan which type of request is pending, and ask your prescriber’s office for the submission date.
Can my plan require a 90-day supply?
Some plans push maintenance medications toward 90-day or mail-order fills. Watch the arithmetic: Cigna’s home-delivery cap for a once-weekly patch is 12 patches per 84 days, which is 84 days of therapy, not 90 — plans often use “90-day” as the name of the benefit while billing an 84-day supply on a product packaged in 28-day cycles. Before you switch, ask what quantity and days supply will actually be billed.
Is the estradiol patch cheaper without insurance?
Sometimes — especially early in the plan year or on a high-deductible plan. But a discount-card purchase generally isn’t credited automatically to your deductible or out-of-pocket maximum, and one made outside the Part D benefit doesn’t automatically count toward the Part D cap. Ask your plan whether a member-submitted claim is allowed, and ask the pharmacy to compare both routes for the same exact fill.
Does insurance cover compounded or “bioidentical” hormone creams?
Compounded hormone products are not FDA-approved — FDA doesn’t review them for safety, effectiveness, or quality before marketing the way it reviews approved drugs. Reimbursement is plan-specific and often limited, so verify with your plan and the dispensing pharmacy rather than assuming either way. → FDA-approved vs. compounded HRT
Did FDA’s label changes change my coverage?
Nothing in the documents we opened shows it. FDA announced the class-wide change on November 10, 2025 and approved the first six updated labels on February 12, 2026 — none of which were estradiol patches. Every payer document we opened was revised after the announcement, and the patch still carries a quantity limit in all of them.
My patch is backordered. Can I appeal that?
No — it’s the wrong tool. An appeal fixes coverage, and a backorder isn’t a coverage problem. Ask whether another manufacturer’s version can be filled, whether another store in the chain has stock, and whether mail order has it. A supply problem needs a phone call, not a form.
Why did my copay go up in January?
Often your deductible reset at the start of the plan year — you’re paying the negotiated price yourself until you meet it again, and a formulary exception can’t waive that. But don’t assume: a January jump can also be a new formulary, a new tier, a pharmacy that left your network, a different manufacturer, or a claim that failed. Ask whether the claim adjudicated and which rule produced the price.
Why is my birth control patch free but my menopause patch isn’t?
Because of federal law, not your insurer. The ACA requires preventive coverage of contraception, so eligible contraceptive products may be covered with limited or $0 cost-sharing when the regulation’s conditions are met at a participating pharmacy. Menopause treatment has no federal mandate. On the same Blue Cross of Illinois list we read, the contraceptive patch carries the ACA-preventive flag while the generic estradiol patch is a non-preferred generic with a quantity limit.
Still not sure which HRT path is right for you?
You don’t have to guess from your insurer’s logo or a one-line message from a pharmacy computer. If you’ve read this far, your next question probably isn’t “is it covered.” It’s “who’s going to help me with this.”
Our free matching quiz weighs your symptoms, whether you have a uterus, your preferred route, your risk history, your insurance situation, and your state — and it tells you when online care isn’t the right starting point at all.
Find My HRT Path
Free · About 90 seconds · No email required to start · How we handle your health data
Find My HRT Path →Sources
- 45 CFR § 156.122 — Prescription drug benefits (category-and-class floor, formulary exceptions, exigent circumstances, timeframes, external review). eCFR, current as of 06/17/2026. https://www.ecfr.gov/current/title-45/subtitle-A/subchapter-B/part-156/subpart-B/section-156.122
- Cigna — National Formulary Coverage Policy: Estrogens (Topical), Patches, Drug Quantity Management. Reviewed 01/05/2026.
- Blue Cross and Blue Shield of Illinois — Performance Drug List, April 2026. https://www.bcbsil.com/il/documents/rx-drugs/drug-lists/performance-il-2026.pdf
- Blue Cross and Blue Shield — Enhanced Drug List, July 2026. https://www.bcbsil.com/il/documents/rx-drugs/drug-lists/enhanced-il-2026.pdf
- Montana Healthcare Programs — Preferred Drug List, revised 01/15/2026. https://medicaidprovider.mt.gov/docs/pharmacy/2026/January2026508CompliantBlackPDL.pdf
- Aetna Medicare FIDE (HMO D-SNP) — 2026 List of Covered Drugs, Illinois. Formulary ID 26010, updated 10/01/2025. https://www.aetna.com/content/dam/aetna/medicaid/illinois-fide-dsnp/pdfs/2026/FORM_2026_26010B24zHMODSNPF_EN.pdf
- CMS — Medicare Part D coverage determinations and exceptions. https://www.cms.gov/medicare/appeals-grievances/prescription-drug/exceptions
- Medicare.gov — Part D costs, 2026. https://www.medicare.gov/health-drug-plans/part-d/basics/costs
- Medicare.gov — What’s the Medicare Prescription Payment Plan? https://www.medicare.gov/publications/12211-whats-the-medicare-prescription-payment-plan.pdf
- KFF — 2025 Employer Health Benefits Survey. Published 10/2025. https://www.kff.org/health-costs/2025-employer-health-benefits-survey/
- Maryland Department of Legislative Services — fiscal and policy note, menopause coverage legislation, 2026 session.
- Maryland Health Care Commission — menopause treatment coverage analysis, December 2025.
- FDA — 2023 First Generic Drug Approvals (estradiol transdermal system 0.014 mg/24hr, Menostar generic, approved 04/17/2023). https://www.fda.gov/drugs/drug-and-biologic-approval-and-ind-activity-reports/2023-first-generic-drug-approvals
- FDA drug shortage database / Drugs.com — Alora discontinuation (03/2021); Menostar generic availability (06/11/2026).
- ASHP Drug Shortage Bulletin (Univ. of Utah Drug Information Service) — estradiol transdermal systems. Updated 07/01/2026.
- FDA announcements — class-wide label change announcement (11/10/2025); first six updated labels approved (02/12/2026).
- Drugs.com price guide — cash prices for two exact fills, retrieved 07/16/2026.
- NPR — Reporting on Jennifer Skoog Mondesir’s experience and CVS confirmation of estrogen patch supply issues, March 2026.