On this page
- Start here — the one-paragraph answer
- The symptom list you've been reading
- Evidence table: what testosterone actually treats
- If it's not testosterone, what is it?
- What actually lowers testosterone in women
- Should I get my testosterone tested?
- Who is testosterone actually right for?
- Is there an FDA-approved testosterone for women?
- FDA-approved treatments for low desire
- Risks and side effects
- Which providers prescribe it?
- Where this evidence is contested
- FAQ
Start here — the one-paragraph answer
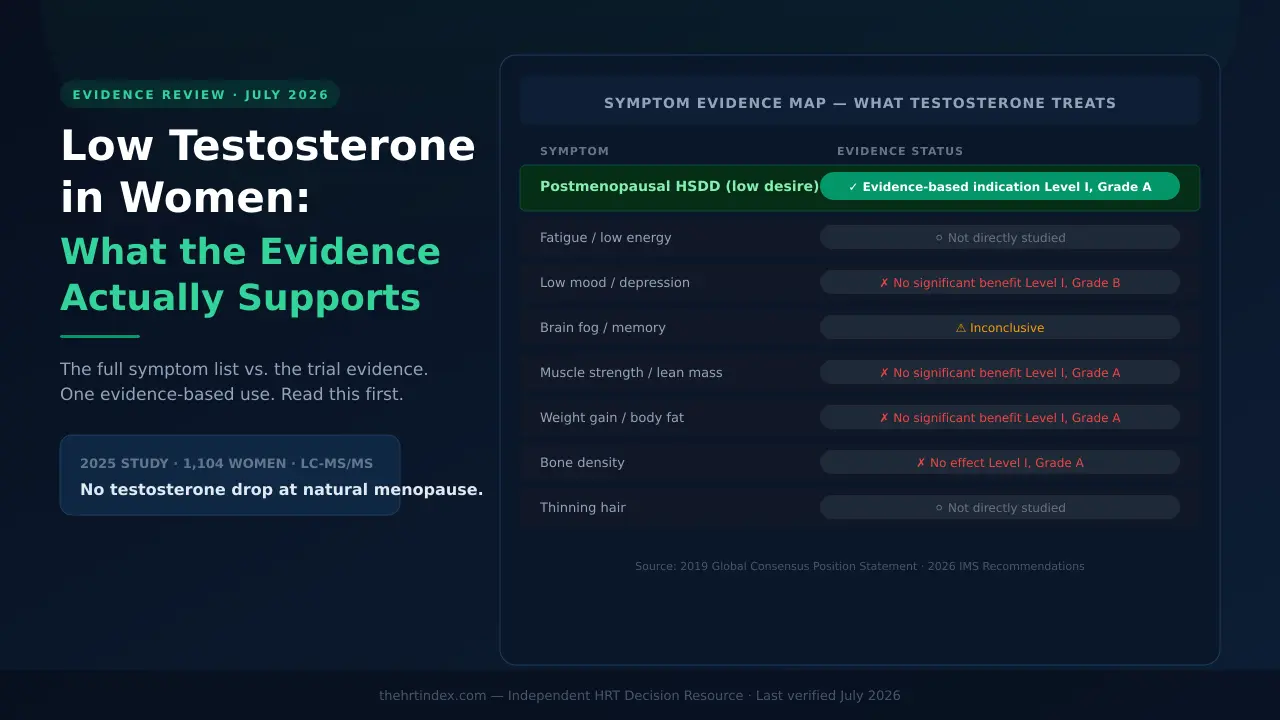
Low testosterone in women symptoms is how the search starts, but the evidence trail leads somewhere specific: testosterone has one clear, evidence-based indication — clinically assessed HSDD (hypoactive sexual desire disorder) in postmenopausal women. For fatigue, brain fog, low mood, muscle weakness, weight gain, and thinning hair, the randomized trials either found no significant benefit or never studied the symptom directly. A 2025 study of 1,104 women found no testosterone drop at natural menopause — debunking the core premise behind most of the marketing. If you're reading this because a clinic offered you testosterone for something other than HSDD, that's the evidence you need before you decide.
What we verified and how
Medical and regulatory claims on this page are traced to the 2026 IMS Recommendations, the 2019 Global Consensus Position Statement (endorsed by 11 international societies), the 2021 ISSWSH Guideline, the 2025 AMY Study (1,104 women, LC-MS/MS), and FDA primary materials. Provider claims are verified from each provider's own published pages, dated July 15, 2026. Editorial conclusions are labeled as ours. Full methodology →
How to read the grades below
| Grade | Level | What it means |
|---|---|---|
| Grade A | Level I | Systematic review of randomized controlled trials — the strongest evidence available |
| Grade B | Level I–II | RCT data with some limitations, or consistent observational data |
| Insufficient | — | Too little data to build a recommendation; not the same as "it doesn't work" |
Source: 2019 Global Consensus Position Statement on the Use of Testosterone Therapy for Women
The low testosterone symptom list you've been reading
Low testosterone in women symptoms as described across the internet: low sex drive, fatigue, brain fog, low mood, muscle weakness, weight gain, and thinning hair. The list appears on clinic websites, consumer articles, and supplement pages with consistent confidence. Here's the problem: the confidence is not coming from the evidence.
The 2019 Global Consensus Position Statement — endorsed by 11 international societies, based on a systematic review of the randomized trial data — addresses most of these symptoms directly. Its conclusions are not what most of the marketing implies.
And the 2025 AMY Study — the largest, most rigorous measurement of female testosterone across the menopause transition, using mass spectrometry in 1,104 women — found no testosterone drop at natural menopause. That finding removes the biological premise the symptom list is usually built on.
Evidence table: what testosterone actually treats in women
Every row below is graded from the trial data. "Not directly studied" is not the same as "disproven" — but it means no RCT has targeted that symptom, and "I felt better" is not the same as a controlled effect.
| Symptom / concern | What the trial evidence shows | Grade |
|---|---|---|
| Sexual desire (HSDD) — postmenopausal | Significant improvement in satisfying sexual events, desire, and arousal in postmenopausal women | Level I, Grade A |
| Fatigue / low energy | Not directly studied as a treatment target. General wellbeing: no significant benefit | Not studied / no benefit |
| Low mood / depression | No statistically significant benefit for mood or depression measures | Level I, Grade B |
| Brain fog / cognitive performance | Too limited to support a recommendation for cognitive performance or delay of decline | Insufficient |
| Muscle strength / lean mass | No statistically significant benefit at physiologic doses | Level I, Grade A |
| Weight gain / body fat | No statistically significant benefit for total body fat or lean body mass | Level I, Grade A |
| Bone density | No effect on bone mineral density at 12 months | Level I, Grade A |
| Thinning hair | Not directly studied as a primary treatment target in these trials | Not studied |
| Vaginal dryness / GSM | Not an established routine treatment for GSM. Vaginal estrogen is FDA-approved for it | Not established |
| Sexual desire — premenopausal HSDD | 2026 IMS: insufficient evidence for routine prescribing. 2021 ISSWSH: more permissive for selected late-reproductive-age women | Insufficient / contested |
Sources: Davis SR, et al. Global Consensus Position Statement. J Clin Endocrinol Metab. 2019;104(10):4660-4666. Islam RM, et al. Safety and efficacy of testosterone for women. Lancet Diabetes Endocrinol. 2019;7(10):754-766. 2026 IMS Recommendations, International Menopause Society.
The honest size of the win for HSDD
For postmenopausal women with HSDD, the evidence is real — but it's worth knowing what the magnitude looks like. A 2019 meta-analysis of 36 randomized trials found testosterone produced approximately 0.85 more satisfying sexual events per month compared to placebo. That's a real, statistically significant effect. It's also not a dramatic transformation for every woman who tries it.
The consensus is also candid: endogenous testosterone levels do not reliably predict who will respond. A low result doesn't mean testosterone will help you, and a result inside the reference interval doesn't mean it won't. The decision is clinical, not numerical.
Everything I believed about this just moved. What applies to me?
Find My HRT Path → free 90-second quiz
Maps your symptoms, menopausal stage, medications, and history to a focused question list for your clinician. Free. No email. Nothing stored. Answers never leave the page.
The 2025 AMY Study: the data that moved the needle
The AMY Study (Australian Women's Midlife Years Study) published in 2025 is the largest, most rigorous cross-sectional measurement of female testosterone across midlife that exists. Key features: 1,104 women aged 40-65, mass spectrometry (LC-MS/MS), not a standard immunoassay.
Its three most important findings:
Finding 1
Testosterone did not differ by menopausal stage among women aged 48-53. Natural menopause itself did not produce an acute testosterone drop.
Finding 2
Testosterone declined about 25% from age 40 to 58-59 — then rose modestly. This is an age effect, not a menopause effect. The "50% by age 40" claim circulating on clinic websites is not supported by this data.
Finding 3
Age, BMI, and smoking together explained only 2.6% of the variation in testosterone between women. That number tells you how little a single lab result tells you about whether your symptoms are testosterone-driven.
The reference range problem
The AMY researchers stated this explicitly in their limitations: because LC-MS/MS assays are not harmonized between labs, the values they published should not be used as reference ranges for other assays. Read that again. The researchers who produced the best female testosterone data in the world explicitly told you not to use their numbers as a reference range. Meanwhile, commercial hormone sites publish tidy "normal testosterone by age" charts as if the number means the same thing everywhere. That's why you won't find one of those charts on this page.
If it's not testosterone, what is it?
Three separate studies from 2025 converge on the same point, using three different methods. The Lancet Diabetes & Endocrinology cross-sectional symptom data from the AMY Study showed which symptoms actually cluster with menopause. The eBioMedicine testosterone paper showed which hormone changes actually occur. The Global Consensus meta-analysis showed which symptoms testosterone actually treats. Put all three together and the picture is coherent: most of the symptom list belongs to a different conversation.
| Symptom | More likely causes | Where to look |
|---|---|---|
| Hot flashes / night sweats | The clearest menopause signal in the AMY data — about 5x more prevalent in perimenopause | Menopause evaluation. This is the #1 FDA-approved reason to use menopausal hormone therapy |
| Vaginal dryness / painful sex | GSM (~2.5x more prevalent in perimenopause). Also: vulvar skin conditions, pelvic floor dysfunction, infection | Vaginal estrogen and GSM → |
| Fatigue | Night sweats disrupting sleep, thyroid disease, iron deficiency or anemia, sleep apnea (under-recognized in midlife women), depression, medications | Depends on your history; see below |
| Brain fog / memory | Fragmented sleep, mood, thyroid, stress load, medications | Mood and cognition → · Sleep → |
| Low mood / irritability | Perimenopausal mood change, depression, sleep debt, thyroid | Mood → |
| Weight gain | Age-related muscle loss, activity, sleep, thyroid, insulin resistance | Symptom-specific evaluation |
| Thinning hair | Thyroid, iron deficiency, androgenetic alopecia | Hair loss → |
| Low libido | Could genuinely be HSDD if postmenopausal and distressing. But also: GSM (painful sex), SSRIs, oral menopausal estrogen raising SHBG, relationship strain, depression, night sweats | Libido and HSDD → |
These are evaluation categories, not diagnoses, and not a test panel to demand. Which ones are relevant depends on your history, your medications, your bleeding pattern, your surgical history, and what's actually bothering you most.
Why estrogen is often the better conversation
On November 10, 2025, the FDA requested labeling changes for menopausal hormone therapies. On February 12, 2026, the FDA approved revised labeling for six of those products — removing boxed-warning language about cardiovascular disease, breast cancer, and probable dementia. Those actions covered estrogen and estrogen/progestogen products.
Read this next part twice — a lot of people are getting it wrong right now
None of that applied to testosterone. There is still no FDA-approved testosterone product for women in the US. The evidence base for testosterone in women did not change in November 2025 or February 2026.
Separately, in 2025 the FDA added a class-wide blood pressure warning to the labels of approved testosterone products, after ambulatory monitoring studies confirmed increases. So if you arrived thinking "hormones are safe now, so testosterone must be fine" — that inference doesn't hold. Estrogen got the good news. Testosterone got a new warning.
What a clinician might check first
Depending on your history, a clinician may consider looking at:
- Thyroid function
- Ferritin and CBC — iron deficiency is common in perimenopause when bleeding can get heavy, and it can produce fatigue, brain fog, and hair loss all at once
- Sleep — including screening for sleep apnea
- Mood
- Your current medications
- Whether your hot flashes and vaginal symptoms are actually being treated
None of that is required for every reader, and a clean result on all of it doesn't automatically mean testosterone is the answer. But if you've been told "your labs are normal" and nobody checked your ferritin, that's a fair thing to ask about.
Not sure whether this is an estrogen or a testosterone conversation?
Find My HRT Path → free 90-second quiz
Maps your symptoms, age, medications, and route preferences — and tells you when you should see someone in person first. Free. No email, no account, nothing stored.
What actually lowers testosterone in women
The main causes are age, having both ovaries removed, and medication effects — including the one almost nobody mentions: oral estrogen raises SHBG, a protein that binds testosterone and changes how your results read. Natural menopause has not been shown to lower testosterone.
SHBG is sex hormone-binding globulin — a protein in your blood that binds a large share of your testosterone. Bound testosterone is still circulating; it just isn't free. When something raises your SHBG, the balance between total and free testosterone shifts, and that changes how your lab result should be read.
| Medication or event | Effect on SHBG | Effect on testosterone |
|---|---|---|
| Oral estrogen (pill you swallow) | Raises it — more than transdermal | Lowers the free fraction |
| Transdermal estrogen (patch, gel, spray) | Much less effect | Free fraction largely preserved |
| Combined oral contraceptive pill | Raises it significantly | Free testosterone falls roughly twice as much as total testosterone (Zimmerman et al., 2014) |
| Ageing | — | Gradual: about 25% from age 40 to 58-59, then modestly back up |
| Natural menopause | — | No stage-related difference detected (AMY Study, 2025, women aged 48-53) |
| Both ovaries removed (bilateral oophorectomy) | — | Yes, measurably. Median 0.33 vs 0.45 nmol/L (p < 0.001, adjusted for age, BMI, smoking) — AMY Study, 2025 |
Sources: Zimmerman Y, et al. Hum Reprod Update. 2014;20(1):76-105. The Menopause Society, 2022. Wang Y, et al. eBioMedicine. 2025;121:105972.
The question worth asking before you buy anything
The Menopause Society's 2022 position statement says that if sexual function or libido is a concern, transdermal estrogen may be preferable to oral estrogen — specifically because it has less effect on SHBG and free testosterone. The 2021 ISSWSH guideline makes a similar point where raised SHBG is relevant.
If you're taking oral menopausal estrogen and your libido has disappeared, ask your clinician whether route and SHBG are relevant to your situation before you pay for anything else.
We're being blunt about why that box is here. If asking that question solves your problem, we make nothing. No visit, no prescription, no commission. Nobody puts this front and centre because there's no product attached to it.
Critical exception — please don't skip this
If you're on combined hormonal contraception, this is a completely different decision. A menopausal estradiol patch is not contraception. Swapping one for the other without a separate pregnancy-prevention plan is not a route change — it's stopping your birth control. Any contraceptive change is its own conversation with your clinician.
Hysterectomy and ovary removal are not the same thing
This trips up an enormous number of women, and the internet is not helping.
A hysterectomy removes your uterus. It does not necessarily remove your ovaries.
A bilateral oophorectomy removes both ovaries. That's the one with the measurable testosterone difference.
You can have a hysterectomy and keep both ovaries. You can have a hysterectomy with a bilateral oophorectomy at the same time. The AMY Study excluded women who'd had both ovaries removed from its main analysis for exactly this reason, then analysed them separately, where the testosterone difference showed up clearly.
If your symptoms started after surgery, get your operative report before your appointment. Not what you remember being told. The document. "I had a hysterectomy" and "I had both ovaries removed" are two different medical situations with two different hormone conversations.
Other conditions that can alter the picture
- Premature ovarian insufficiency — ovaries stopping early
- Adrenal insufficiency — your adrenal glands make androgen precursors too
- Hypopituitarism — a pituitary problem changes the whole picture
- Anti-androgen medications — spironolactone and finasteride, among others, can alter how androgens act or are metabolized
Those aren't self-diagnosis material. They're reasons to see a clinician in person rather than start a subscription.
Should I get my testosterone tested?
A testosterone result cannot diagnose HSDD or prove that fatigue, brain fog, weight change, or low mood are caused by testosterone. No blood level designates female testosterone deficiency, and most routine immunoassays lack precision at the concentrations found in women. Testing is genuinely useful for three narrower things: documenting a baseline before treatment, spotting an unexpectedly high value, and monitoring treatment so levels don't run too high.
| What you'll often read | What current guidance actually says |
|---|---|
| "Normal is 15-70 ng/dL; below that is low" | No blood level designates female testosterone deficiency. No cutoff for any circulating androgen separates women with sexual dysfunction from women without it |
| "A simple blood test measures your levels" | Most routine immunoassays lack precision in the female range. LC-MS/MS is preferred where accurate low-concentration measurement matters |
| "Get tested to find out if you have low T" | A blood testosterone level should not be used to diagnose HSDD. The diagnosis is clinical — a full assessment, not a number |
| "Check your free testosterone" | Research should focus on total testosterone. Evidence that the free fraction is the biologically active one is lacking |
What a "low" result actually means
It means the value your sample produced was below the reference interval for that lab's assay. That's it. That's the whole claim.
It does not mean testosterone is causing your symptoms. It doesn't mean you have a deficiency syndrome. And it doesn't predict whether testosterone would help you — endogenous testosterone levels don't reliably predict who responds.
Bring the whole report to your appointment: result, units, reference interval, date, method, whether it's total or free, SHBG if measured, and why the test was ordered. The number without that context isn't much of a number.
So why does any good provider test at all?
Because a testosterone measurement has two real jobs:
- Documenting a baseline before treatment — including catching an unexpectedly high starting value. Midi, for example, lists testosterone above 100 ng/dL as a reason not to prescribe.
- Monitoring during treatment, so you don't drift into supraphysiologic levels. The consensus recommends a baseline before starting, a recheck at 3-6 weeks, then periodically.
Notice what's not on that list: ruling out thyroid disease, iron deficiency, or sleep apnea. The testosterone result doesn't do that. Your history, your examination, and separate targeted tests do.
A clinic should not use a testosterone cutoff by itself to diagnose HSDD or decide whether you're eligible — because no such validated cutoff exists. Baseline testing as one part of a broader clinical assessment is completely appropriate. A number used as a gate is not.
Are at-home testosterone tests good enough?
Not for deciding whether you have "low T" — and not for the reason you'd expect. The collection isn't really the issue. The issue is everything around it: which assay ran it, what reference interval it's being compared against, and what decision the result would actually change.
The real risk isn't a wrong number. It's a right number, misread. You get a result flagged "low," it finally feels like an explanation, and you spend the next year treating the wrong thing while your ferritin sits at 8 and nobody's looked.
You've got a number, or symptoms, and no idea what to ask
Find My HRT Path → free 90-second quiz
Turns what you're experiencing into a focused question list for your first consult — including which assay to ask about and which other causes to raise. Free. No email. Nothing stored. Answers never leave the page.
Who is testosterone for women actually right for?
Testosterone has clear evidence for a specific woman: postmenopausal, with sexual desire that is persistently low and genuinely distressing, where a proper assessment has considered the other contributors — pain, GSM, medications, mood, sleep, and relationship factors. If that's you, the evidence is real and you deserve access to it. If it isn't, it isn't.
What is HSDD — and how is it actually diagnosed?
HSDD is hypoactive sexual desire disorder: sexual desire that's persistently or repeatedly low, causes you marked distress or difficulty in your relationship, and isn't better explained by another medical or psychiatric condition, a relationship problem, a medication, or another substance.
Three things follow from that definition, and they're the three things clinics gloss over:
- The distress is part of the diagnosis. If your desire is lower and you're at peace with it, that isn't HSDD. That's a life change, and it doesn't need a prescription.
- The exclusion step is part of the diagnosis. "Not better explained by something else" is doing real work. If sex hurts, or you're on an SSRI, or you haven't slept properly in two years — that has to be addressed as part of the assessment, not waved past.
- No blood test makes this diagnosis. It's clinical. A number can't confirm it and a number can't rule it out.
You're likely a fit if
- ✅ You're postmenopausal — natural or surgical — and
- ✅ Your sexual desire is persistently low and it distresses you — and
- ✅ The other contributors — pain, GSM, vasomotor symptoms, sleep, medications, mood, relationship factors — have been assessed and addressed where they're relevant
You're likely not a fit if
We're going to tell you to leave. Most pages won't. Here's who should:
- ❌ You're premenopausal. The 2026 IMS Recommendations find insufficient evidence to support routine testosterone prescribing for premenopausal HSDD. Perimenopause symptoms checklist →
- ❌ Your main complaint is fatigue, brain fog, weight, or mood. Trials found no significant benefit for these outcomes. Mood and cognition → · Sleep →
- ❌ Sex hurts. GSM is a common cause. Testosterone is not an established routine treatment for GSM. Vaginal estrogen is FDA-approved for it. Vaginal estrogen and GSM →
- ❌ You want it for bone or muscle. No effect on bone density at 12 months. No significant benefit for lean mass or strength. HRT benefits and risks →
- ❌ You have a history of hormone-sensitive breast cancer. Women with prior breast cancer were excluded from the trials. The safety findings don't cover you. See a clinician in person.
- ❌ You're at high cardiometabolic risk. Also excluded from the trials.
These need urgent or direct clinical evaluation — not a subscription
- 🚩 Suicidal thoughts, or a mental health crisis — please contact emergency services or a crisis line now. In the US, call or text 988
- 🚩 Chest pain, severe shortness of breath, or new neurological symptoms — emergency care
- 🚩 Unexplained bleeding after menopause — needs evaluation, promptly
- 🚩 A rapidly deepening voice, or fast-developing male-pattern hair changes — that's a "find out why" signal, not a "start testosterone" signal
- 🚩 A new severe headache with vision changes — could point to a pituitary problem
- 🚩 Symptoms that started right after major surgery, where nobody has reviewed your operative report
- 🚩 Pregnancy, or active fertility treatment
Is there an FDA-approved testosterone for women?
No. There has never been an FDA-approved testosterone product for women in the United States. Every woman using testosterone in the US is using either a product approved for men, prescribed off-label at a much lower dose, or a compounded preparation. A women-specific testosterone formulation is approved in Australia, the United Kingdom, New Zealand, and South Africa — but not in the US.
The timeline nobody puts in one place
| Year | What happened |
|---|---|
| 2004 | Intrinsa (testosterone patch for HSDD after surgical menopause) rejected by FDA after advisory committee raised long-term safety concerns. Later approved in Europe for a narrower population, then withdrawn by manufacturer. |
| 2011 | LibiGel (testosterone gel) missed Phase III endpoints — not because it did nothing, but because placebo did almost as much. High placebo response attributed to frequent study visits, diary reminders, and expectation. That detail is the tell: desire is strongly placebo-responsive. |
| 2025 | FDA adds a class-wide blood pressure warning to all approved testosterone product labels, after ambulatory monitoring studies confirmed increases. |
| Today | A women-specific testosterone product is approved in Australia, the UK, New Zealand, and South Africa. In the US: still nothing with a female indication. |
Testosterone is a Schedule III controlled substance
Testosterone is a Schedule III controlled substance in the United States. It requires a valid prescription from a licensed clinician. Under federal law, an authorized Schedule III prescription may be refilled up to five times within six months. Current federal telemedicine flexibilities remain in effect through December 31, 2026.
If a website offers you testosterone without a prescription, or without a genuine clinical evaluation, stop there. That's not a shortcut. That's a different category of problem.
Compounded is not FDA-approved. Ever.
Compounded drugs are not FDA-approved. The FDA does not review their safety, effectiveness, or quality before they are marketed.
Not "less rigorously." Doesn't. A compounded testosterone cream has not been through FDA premarket review. The FDA has specifically flagged describing compounded preparations as FDA-approved or as "clinically proven" as misleading in its guidance to telehealth companies.
And here's the genuine tension: the Global Consensus recommends against compounded testosterone — and acknowledges that where no approved female product exists, a compounded product may be needed, in which case the compounding pharmacy should meet Good Manufacturing Practice standards. In the US, both halves of that sentence apply at once. That's not a loophole. It's an unresolved regulatory gap.
Pellets: the one thing the consensus is unambiguous about
The Global Consensus recommends against any preparation that produces supraphysiologic testosterone concentrations — specifically including pellets and injections — and states that its efficacy findings do not apply to them.
Pellets are implanted under the skin. The dose can't be adjusted after insertion. Removal may require another procedure and may not reverse your exposure quickly. If a clinic leads with pellets, that tells you what you need to know about the clinic.
Are there FDA-approved treatments for low desire that aren't testosterone?
Yes — two. This is a fact that deserves to be on the page:
There is no FDA-approved testosterone for women.
But there are two FDA-approved prescription medications for HSDD.
They're just not the ones the hormone clinics are selling.
| Addyi (flibanserin) | Vyleesi (bremelanotide) | Testosterone | |
|---|---|---|---|
| FDA-approved for HSDD? | Yes | Yes | No female indication |
| Approved population | Acquired, generalized HSDD; women under 65, including naturally postmenopausal women under 65 | Acquired, generalized HSDD; premenopausal women | — |
| Where the evidence points | Approved indication | Approved indication | Evidence-based use in postmenopausal HSDD — but off-label or compounded |
"Acquired" means the low desire is a change from how you used to be. "Generalized" means it isn't limited to one partner or one situation. We're not recommending either — each has its own contraindications and side-effect profile, and those conversations belong with a clinician who knows your history. What we're telling you is that the menu is bigger than the one you've been shown.
What are the risks and side effects of testosterone for women?
In randomized trials of selected, generally lower-risk postmenopausal women taking physiologic doses over limited follow-up, testosterone did not increase serious adverse events. The realistic side effects are mild acne and increased body or facial hair. The bigger issues are what the data doesn't cover: women at high cardiometabolic risk were excluded, and randomized safety evidence beyond 24 months is not established.
| Concern | What the evidence shows | Grade |
|---|---|---|
| Acne, body or facial hair | Mild increases in some women | Level I, Grade A |
| Hair loss, clitoral enlargement, voice change | Not associated at physiologic doses | Level I, Grade A |
| Oral testosterone (swallowed) | Adverse effects on cholesterol — not recommended | Level I, Grade A |
| Non-oral (patch, gel, cream) | No significant short-term cholesterol effects | Level I, Grade A |
| Blood pressure | Female trials: no statistically significant increase in selected populations over limited follow-up. Separately: FDA added a class-wide blood pressure warning to approved testosterone product labels in 2025 | Level I, Grade A (female trials); FDA 2025 (label warning) |
| Blood sugar, HbA1c | No increase in the populations studied | Level I, Grade A |
| Blood clots | Non-significant trend toward increased risk. The role of estrogen taken alongside can't be excluded | Level I, Grade A |
| Breast density | No increase | Level I, Grade A |
| Breast cancer, short-term | Transdermal doesn't appear to affect risk | Level I, Grade A |
| Breast cancer, long-term | Insufficient data | Insufficient |
| Beyond 24 months | Randomized safety evidence not established | Level I, Grade A |
The two-year wall
If you start testosterone at 52 and use it for ten years, at month 25 you are beyond the randomized safety evidence. That's not scaremongering. It's the consensus's own boundary, and it applies to a therapy many women are encouraged to plan on indefinitely. It doesn't mean don't. It means know.
The stop rule
Current IMS guidance: benefits generally begin to emerge after four to six weeks, and if there's no significant benefit by six months, stop. Not increase the dose. Stop.
The treatment plan should define the target outcome and the reassessment schedule at the start. A provider who can't tell you what they're measuring and when they'll decide isn't following the guidance. That's a first-visit question, not a fifth-visit question.
Which online providers actually prescribe testosterone to women?
Fewer than you'd think. Of the major women's telehealth platforms, Midi Health publishes a testosterone program using a compounded cream, requiring lab work and typically two visits before a prescription. Winona states it does not prescribe testosterone. Hers does not list testosterone on its current perimenopause treatment page. All verified July 15, 2026.
Disclosure: The HRT Index has active affiliate relationships with Hers, Midi Health, Winona, and Sesame. This page contains one compensated outbound link — to Midi Health — and we may earn a commission if you start care through it, at no extra cost to you. Affiliate status does not determine the editorial findings on this page. The audit below is how you check that.
| Provider | Prescribes testosterone? | FDA status | Labs? | Insurance? | Verified |
|---|---|---|---|---|---|
| Midi Health | Yes — compounded cream (testosterone USP, micronized), applied to skin | Compounded — NOT FDA-approved. Per Midi's own disclosure, FDA does not evaluate compounded medications for safety, effectiveness, or quality prior to use | Yes. Labs at treatment start and again at 4-6 weeks; clinician may recommend checks every 6-12 months | Bills insurance for visits. Compounded medications cannot be covered by insurance (Midi's own Custom Rx page) | Jul 15, 2026 |
| Winona | No — "Currently, we do not prescribe testosterone" (their FAQ, verbatim). Offers compounded oral DHEA | Estradiol patches, estradiol tablets, and progesterone capsules are FDA-approved per Winona's disclosure; compounded creams and oral DHEA are not | No bloodwork required — states this aligns with The Menopause Society and ACOG | Does not bill insurance. HSA/FSA accepted | Jul 15, 2026 |
| Hers | Not listed on current perimenopause treatment page, which covers estradiol (oral and patch), progesterone, and estradiol vaginal cream | Estradiol / progesterone | — | — | Jul 15, 2026 |
Excluded from this comparison: Sesame and Inner Balance (Oestra). We could not verify their testosterone prescribing policies as of July 15, 2026, so we're not publishing rows for them. An empty row and a verified row shouldn't look alike.
The audit: where provider claims outrun the evidence
Midi and Winona are both HRT Index affiliate partners. We publish this anyway. If we didn't, nothing else on this page would be worth much.
| Claim | Who says it | What we verified | Verdict |
|---|---|---|---|
| "By menopause, women can lose up to 50% of their natural testosterone" | Midi | Midi's cited source is a Cleveland Clinic consumer page — one of the sources the 2025 AMY Study names when describing the claim it went on to test. The AMY data found no stage-related testosterone difference across menopause and a 25% decline from age 40 to 58-59, not 50% by 40 | Not supported |
| "by age 40, most women have lost up to 50%" | Midi (store page) | Same citation chain. The AMY data shows ~25% decline from age 40 to 58-59 — across nearly 20 years, not by age 40. The store page claim is more aggressive than the program page claim, using the same source | Not supported |
| Testosterone is offered with monitoring at 4-6 weeks | Midi (program page) | The program page says 4-6 weeks; the blog elsewhere mentions 8-12 weeks. Not reconciled on the pages we read. We're noting the contradiction; we didn't enroll | Contradicted |
| Testosterone "safely" prescribed premenopausally | Midi (blog) | The 2026 IMS Recommendations find insufficient evidence to support routine testosterone prescribing premenopausally. Midi's blog frames it as safe without naming which guideline it's based on | Unsupported |
| "Does not prescribe testosterone" | Winona | Verified verbatim in their FAQ. We're reporting what they state. Rated high-change-risk: if Winona expands their formulary, this row changes | Verified |
The honest assessment of Midi — including the parts that cost us the sale
Midi does NOT give you testosterone after one visit. If speed is your priority, plenty of clinics will hand you a same-day script — Midi is the wrong choice and we say so. But because Midi skips the fast track, the extra visit and lab review create the chance to look at the thyroid, the ferritin, the oral estrogen raising your SHBG — before you spend a year treating the wrong thing.
That process doesn't guarantee they'll catch those things — we didn't enroll and can't verify execution. It creates the opportunity. For the subset of women who genuinely recognize themselves in the HSDD profile and want careful, monitored care, that's worth knowing.
You recognize yourself in the HSDD profile — can you actually get care?
Affiliate link. We may earn a commission if you start care through this link, at no extra cost to you. Midi prescribes compounded testosterone — not FDA-approved. Verified July 15, 2026.
Where this evidence is contested
Not everyone accepts the reading on this page. A minority of clinicians and researchers argue the trials were too short, measured the wrong things, and applied a standard of evidence to women that was never applied to men. That argument deserves a fair hearing, so here it is — made as well as we can make it, not as a straw man.
The case for a more permissive view
The double standard is real, and it's hard to wave away. There are many FDA-approved testosterone products for men and none with a female indication. Critics — including researchers who worked on the female testosterone trials themselves — have argued this reflects how seriously men's and women's sexual health are taken, not a difference in the evidence.
The trials may have measured the wrong thing. The consensus itself recommends that "satisfying sexual events" should no longer be used as the primary measure, and notes that no existing questionnaire captures every domain of female sexual function. If the yardstick is wrong, "no significant benefit" findings are weaker than they look.
"Insufficient" is not "it doesn't work." For premenopausal women and for cognition, the evidence is too limited to build a recommendation on — not the same as a finding of no effect.
| Question | 2026 IMS Recommendations | 2021 ISSWSH Guideline |
|---|---|---|
| Postmenopausal HSDD | Evidence-based indication for a monitored trial | Supported |
| Premenopausal HSDD | Insufficient evidence to support routine prescribing | More permissive for selected late-reproductive-age women, on limited data |
If a provider tells you testosterone is fine premenopausally, they may be leaning on ISSWSH. That's a defensible position to argue, but it isn't the current IMS position, and you're entitled to know there's a disagreement rather than be told it's settled.
One disclosure we think you should have
Susan Davis — lead author of the Global Consensus Position Statement and senior author of the 2025 AMY Study — discloses that she has served on advisory boards for Besins Healthcare and has received institutional research funding and trial drug supply from Lawley Pharmaceuticals, which makes a testosterone product for women.
A disclosed financial relationship is neither evidence for nor against a study's findings. It's a potential conflict you're entitled to know about, and it's a reason to look at the methods — not a reason to dismiss the work. We're flagging it because nobody else on the first page of results did.
Editorial conclusion — labeled as such
We think both things are true at once. The evidentiary bar for women's sexual health has been unfairly high — and the pooled trial data does not support testosterone for fatigue, mood, cognition, muscle, fat, or bone. The first injustice doesn't make the second finding disappear. Being angry about the double standard is completely reasonable. Buying a compounded cream for your brain fog is a different decision, and the anger doesn't make it work. Where the evidence is contested, we've told you. Where it's Grade A, we've told you that too. You get to weigh it. That's the entire point of this page.
How we researched and verified this page
This page is editorial research. It is not medical advice, and it has not been reviewed by a clinician. Medical and regulatory claims are traced to current guidelines, FDA materials, prescribing information, or peer-reviewed research. Provider claims are labeled separately as provider-stated commercial facts and dated to the page we read. Editorial conclusions are labeled as ours.
We separate three kinds of statement:
- Medical or regulatory fact — sourced to primary or authoritative material. Never to a competitor's blog.
- Verified commercial fact — read on the provider's own live page, with the date we read it.
- Editorial conclusion — our judgment, based on the facts above, labeled so you can disagree with it.
What we didn't do: We didn't enroll. We didn't order. We haven't tested any product. We can't tell you how any provider's published process performs in real life, and you should be suspicious of any affiliate site that claims otherwise. Full methodology →
Frequently asked questions
What are the symptoms of low testosterone in a woman?
The symptoms usually attributed to it are low sex drive, fatigue, brain fog, low mood, muscle weakness, weight gain, and thinning hair. None of them diagnose low testosterone. Current guidance supports one evidence-based use for testosterone in women: clinically assessed HSDD in postmenopausal women. Several other symptoms on the standard list were never studied as treatment targets at all.
What is a normal testosterone level for a woman?
Laboratories publish assay-specific reference intervals, but there is no universal serum testosterone cutoff that diagnoses HSDD, proves symptoms are caused by testosterone, or establishes a female testosterone-deficiency syndrome. Interpret a result using the assay, units, reference interval, your symptoms, your medications, and the reason the test was ordered.
Does testosterone drop at menopause?
Current evidence does not show an acute testosterone drop caused by natural menopause. In a 2025 cross-sectional study of 1,104 women measured by mass spectrometry, testosterone did not differ by menopausal stage among women aged 48-53. It declined with age about 25% between ages 40 and 58-59, then rose modestly. The authors concluded the data do not support menopause itself as a reason for testosterone supplementation.
Can a woman have low testosterone symptoms with a normal blood result?
Yes, because those symptoms have many possible causes, and most of them have nothing to do with testosterone. A result inside the reference interval also doesn't rule out an HSDD assessment, because no blood level defines the condition. HSDD is diagnosed clinically, not by a number.
Can a woman have a low result without any symptoms?
Yes. A low value on its own doesn't establish a deficiency syndrome or create a reason to treat. Age, BMI and smoking explained only 2.6% of the variation in testosterone between women in the 2025 AMY Study, so a single number sitting below a reference interval tells you much less than it appears to.
Does a low result mean testosterone will help me?
No. Endogenous testosterone levels don't reliably predict who responds to treatment, which is one reason no cutoff is used to decide eligibility. Whether testosterone is appropriate depends on a clinical HSDD assessment, not on where your number falls.
Can low testosterone cause fatigue in women?
There's no good evidence that testosterone treats fatigue. It wasn't directly studied as a treatment target, and the nearest measured outcome, general wellbeing, showed no significant benefit. Sleep disruption, thyroid disease, iron deficiency, medications, and mood are more common explanations and are usually easier to check.
Can low testosterone cause weight gain in women?
The trials don't support treating it with testosterone. Testosterone showed no statistically significant benefit for total body fat or lean body mass at physiologic doses (Level I, Grade A).
Does testosterone help with brain fog in women?
The evidence is inconclusive. The Global Consensus found the evidence too limited to support testosterone for improving cognitive performance or delaying cognitive decline in postmenopausal women. Inconclusive means what exists isn't good enough to build a recommendation on, not that it's been tested and failed.
Is testosterone FDA-approved for women?
No. There has never been an FDA-approved testosterone product for women in the United States. Women who use it receive either a product approved for men, prescribed off-label at a lower dose, or a compounded preparation. A women-specific testosterone formulation is approved in Australia, the United Kingdom, New Zealand, and South Africa.
Are there FDA-approved medications for low sexual desire?
Yes. Addyi (flibanserin) is FDA-approved for acquired, generalized HSDD in women under 65, including naturally postmenopausal women under 65. Vyleesi (bremelanotide) is FDA-approved for acquired, generalized HSDD in premenopausal women. Neither is testosterone, and neither replaces a clinical HSDD assessment.
Did the FDA's 2025-2026 hormone therapy changes apply to testosterone?
No. On November 10, 2025 the FDA requested labeling changes for menopausal hormone therapies, and on February 12, 2026 it approved revised labeling for six products, removing boxed-warning language about cardiovascular disease, breast cancer, and probable dementia. Those actions concerned estrogen and estrogen/progestogen products. Separately, in 2025 the FDA added a class-wide blood pressure warning to approved testosterone product labels.
Does a hysterectomy lower testosterone?
It depends entirely on whether your ovaries were removed. A hysterectomy removes the uterus; it does not necessarily remove the ovaries. Removing both ovaries does measurably lower testosterone: in the 2025 AMY Study, postmenopausal women who had both ovaries removed had a median testosterone of 0.33 nmol/L versus 0.45 nmol/L in postmenopausal women with at least one ovary. Get your operative report and find out which surgery you had.
Can I get testosterone if I'm premenopausal?
Some providers prescribe it. The 2026 IMS Recommendations find insufficient evidence to support routine testosterone prescribing for premenopausal HSDD, while the 2021 ISSWSH guideline is more permissive for selected late-reproductive-age women based on limited data. That's a live disagreement between guidelines. If a provider tells you it's simply safe premenopausally, ask which guidance that's based on.
Can low testosterone cause vaginal dryness?
Vaginal dryness commonly warrants evaluation for genitourinary syndrome of menopause (GSM), though vulvar skin conditions, pelvic floor dysfunction, and infection may also need ruling out. Low-dose vaginal estrogen is FDA-approved for GSM. Testosterone is not an established routine treatment for it. Dryness can reduce desire indirectly, if sex hurts you avoid it, but treating that with testosterone targets the wrong problem.
What type of doctor checks testosterone in women?
A gynecologist, a certified menopause practitioner, a primary care clinician, an endocrinologist, or a sexual medicine specialist, depending on your main concern. For distressing low desire, a menopause or sexual medicine clinician is the best fit. For a suspected pituitary, adrenal, or ovarian problem, that's an endocrinologist, and it should be in person.
How long does testosterone take to work, and when should I stop?
Current IMS guidance is that benefits generally begin to emerge after four to six weeks, and that treatment should stop if there's no significant benefit by six months. Not increase the dose. Stop. The target outcome and reassessment schedule should be agreed at the start.
Are testosterone pellets safe for women?
The Global Consensus recommends against any preparation producing supraphysiologic testosterone concentrations, specifically including pellets and injections, and states its efficacy findings don't apply to them. Pellet dosing can't be adjusted after insertion; removal may require another procedure and may not reverse exposure quickly. Midi Health explicitly declines to prescribe pellets for this reason.
Is testosterone a controlled substance?
Yes. Testosterone is a Schedule III controlled substance in the United States and requires a valid prescription. Under federal law, an authorized Schedule III prescription may be refilled up to five times within six months; state law and prescriber policy may be stricter. Federal telemedicine flexibilities remain in effect through December 31, 2026, subject to applicable requirements.
Are at-home testosterone tests worth it?
Not for deciding whether you have low T. An at-home result can't diagnose HSDD or establish that treatment is suitable by itself, and its usefulness depends on the specimen, the collection, the assay, the reference interval, and what decision it's meant to inform. The risk isn't a wrong number, it's a right number, misread, that sends you down the wrong path for a year.
So where does this leave you?
You now have the evidence distinctions and the questions you need for a much more focused conversation with a clinician. The honest summary:
- → If your desire is persistently low, you're postmenopausal, and it genuinely distresses you — testosterone is a real, evidence-backed option for clinically assessed HSDD. Ask about Addyi too.
- → If your main complaints are fatigue, brain fog, weight, or mood — those symptoms don't establish testosterone deficiency. Your next evaluation may need to look at sleep, thyroid, iron, medications, mood, and menopause symptoms.
- → If you're on oral menopausal estrogen — ask whether route and SHBG are relevant before you buy anything.
- → If your symptoms started after surgery — get the operative report. "Hysterectomy" and "both ovaries removed" are not the same thing.
- → If you're premenopausal — the guidelines disagree with each other. Know that going in.
Still not sure which path applies to you?
Find My HRT Path → personalized action plan, free
Maps your symptoms, age, whether you have a uterus, your medication route preference, your risk history, your insurance situation, and your state to the right starting point — and tells you when online care isn't the right first step at all.
No email. No account. Nothing is stored and your answers never leave the page. About 90 seconds. Educational care-path guidance, not a diagnosis.
Sources
- 2026 IMS Recommendations, International Menopause Society.
- Davis SR, Baber R, Panay N, et al. Global Consensus Position Statement on the Use of Testosterone Therapy for Women. J Clin Endocrinol Metab. 2019;104(10):4660-4666. Endorsed by 11 international societies.
- Wang Y, Islam RM, Bond M, Davis SR. Testosterone and pre-androgens by age and menopausal stage at midlife: findings from a cross-sectional study. eBioMedicine. 2025;121:105972. doi:10.1016/j.ebiom.2025.105972. (Open access, CC BY.)
- Islam RM, Bond M, Ghalebeigi A, Wang Y, Walker-Bone K, Davis SR. Symptom prevalence across the menopause transition. Lancet Diabetes Endocrinol. 2025;13(9):765-776.
- Islam RM, Bell RJ, Green S, Page MJ, Davis SR. Safety and efficacy of testosterone for women: a systematic review and meta-analysis of randomised controlled trial data. Lancet Diabetes Endocrinol. 2019;7(10):754-766.
- Parish SJ, Simon JA, Davis SR, et al. ISSWSH Clinical Practice Guideline for the Use of Systemic Testosterone for Hypoactive Sexual Desire Disorder in Women. J Sex Med. 2021;18(5):849-867.
- The 2022 Hormone Therapy Position Statement of The North American Menopause Society. Menopause. 2022;29(7):767-794.
- Zimmerman Y, Eijkemans MJC, Coelingh Bennink HJT, et al. The effect of combined oral contraception on testosterone levels in healthy women: a systematic review and meta-analysis. Hum Reprod Update. 2014;20(1):76-105.
- Handelsman DJ, Davis SR. Measuring serum testosterone in women. Lancet Diabetes Endocrinol. 2024;12(7):437-439.
- US Food and Drug Administration — labeling change request for menopausal hormone therapies (November 10, 2025); approved revised labeling for six MHT products (February 12, 2026).
- US Food and Drug Administration — class-wide labeling changes for testosterone products (2025).
- US Food and Drug Administration — human drug compounding; and FDA & Telehealth Companies: What to Know When Promoting Compounded Drugs (June 2026).
- US Food and Drug Administration — prescribing information, Addyi (flibanserin) and Vyleesi (bremelanotide).
- US Drug Enforcement Administration — controlled substance schedules and refill requirements.
- Midi Health — testosterone program page, store page, Custom Rx page, and blog. Read July 15, 2026.
- Winona — HRT FAQ and DHEA product page. Read July 15, 2026.
- Hers — perimenopause treatment page. Read July 15, 2026.
The HRT Index is the independent menopause HRT decision layer for women. This page is editorial research, not medical advice, and has not been reviewed by a clinician. We have active affiliate relationships with Hers, Midi Health, Winona, and Sesame; this page contains one compensated link, to Midi Health. Last verified July 2026.