The best online menopause clinic for irregular periods is Midi Health for most women. It's available in all 50 states, is in-network with most PPO plans, runs live 30-minute video visits, and its clinicians can order clinically indicated blood work and imaging. But some bleeding patterns need an in-person exam first — and no video visit can deliver that part.
That last sentence is the one nobody selling you a subscription says out loud.
So here's the deal. We checked eight online menopause and telehealth services. There are two things a woman with irregular bleeding often ends up needing: a tissue sample to find out what's happening, and — if the answer is heavy bleeding — the device that treats it best. Neither one can happen on a video call. Not at Midi. Not at the compounded brands. Not at the one paying us the most.
That is not a reason to skip online care. It's a reason to know which half of your problem online care solves — because for most women, it solves the important half. We'll show you which half is yours, and what it costs when it isn't.
Start here — the four routes
| If this is you | Start with | The condition |
|---|---|---|
| Ordinary cycle changes, you have a PPO | Midi Health | $250 self-pay first visit; in-network with most PPO plans; no Medicare or Medicaid |
| You want a doctor-led video visit nationwide | Gennev (we earn nothing) | $250 first visit self-pay; insurance accepted |
| Cash-pay, want ongoing video plus messaging | Sesame | No insurance billing; official starting prices currently disagree — check live |
| Red-flag bleeding, or bleeding after 12 months | In-person evaluation | Not online. Not yet. |
No buttons in this table on purpose. Find your bleeding pattern first — that's the next section.
This answer changes if:
- •You've gone 12+ months without a period and you're bleeding now. See someone in person, soon. ACOG changed this guidance on April 16, 2026: for most patients, the initial evaluation is now an ultrasound and a tissue sample. The tissue sample requires an exam room.
- •You're older than 45 with abnormal bleeding. Online care can start it. But ACOG names endometrial tissue sampling as a first-line test for your age group. Budget for a referral.
- •You're soaking a pad or tampon every hour, bleeding longer than a week, bleeding between periods, or bleeding after sex. Get evaluated in person before starting hormones.
- •You have Medicare or Medicaid. Midi accepts neither. Most of this category doesn't bill insurance at all. Here's what to do instead
- •You want to be seen in person, paying cash. Sesame's marketplace side. It's not a menopause clinic. That's exactly why it works for this.
The HRT Index is the independent decision resource for online menopause and HRT care — comparing telehealth providers on clinical legitimacy, care quality, medication fit, price transparency, and access, with every claim verified and dated, so women can choose the path that fits their situation before their first consult.
The right online HRT provider isn't the same for every woman — it depends on your symptoms, your age and whether you have a uterus, your medication route preference, your risk history, your insurance or cash-pay situation, and your state. Some situations belong with an in-person clinician first. Because a general answer can't resolve those for you, use The HRT Index's Find My HRT Path tool to match your situation to the right provider — and to flag when online care isn't the right starting point — before your first consult.
“Irregular periods” is three different problems wearing one name
“Irregular periods” covers at least three separate clinical situations: ordinary perimenopausal cycle change, abnormal uterine bleeding that warrants evaluation, and postmenopausal bleeding that warrants prompt evaluation. They share a phrase but not a next step. Most comparison pages treat them as one symptom, which is why none of them can tell you which clinic you need.
Start with what's happening in your body. It makes everything after this make sense.
For most of your life, your ovary released an egg each month. After ovulation, the follicle it came from turns into a structure called the corpus luteum, which produces progesterone — a hormone whose job here is to stop your uterine lining from building and tell it when to shed. That's what made your period arrive roughly when you expected it.
Perimenopause is the years-long stretch before your periods stop for good. During it, ovulation gets unreliable. Some months your ovary skips it. When that happens, no corpus luteum forms, so no progesterone shows up — and estrogen keeps building the lining of your uterus, the endometrium, with nothing to end the cycle.
So the lining keeps going. Until it sheds all at once.
That's called anovulatory bleeding, and it's one common reason perimenopausal periods become delayed, prolonged, heavy, or unpredictable. It is not the only reason. Fibroids and polyps — benign growths in or on the uterus — do it too. So do thyroid disease, pregnancy, certain medications, and changes to the endometrium itself. Which is the entire point: “it's just perimenopause” is a conclusion, not a starting assumption, and you can't reach it from a website.
Repeated cycles of estrogen building the lining with no progesterone to end it — what clinicians call unopposed estrogen exposure — can contribute to endometrial overgrowth in some women. That's why your age and your risk factors change the answer.
You didn't come here to be reassured. You came here because you already got reassured, by someone who had twelve minutes, and it didn't help. So we're going to show you where your pattern sits.
What's expected in perimenopause — and what should be evaluated
Cycle changes are the defining feature of perimenopause: cycle length shifting by seven days or more, skipped months, and changes in flow are expected. Bleeding that lasts longer than seven days, arrives more often than every 21 days, follows sex, or occurs 12 or more months after a final period should be evaluated by a clinician rather than assumed to be perimenopause.
One frequently cited chart-review distribution found that among women going through the transition, about 70% had scanty or infrequent periods, about 18% had heavy or otherwise excessive bleeding, and only about 12% stopped menstruating suddenly with no irregular bleeding at all.
The clean version — periods that just space out and stop — is the rare one. Chaos is closer to the rule than the exception. You are not broken and you are not unusual. You are also not automatically fine. Both things are true, and holding both is the whole skill here.
What's expected
- Cycle length moving around. A shift of seven days or more from your usual is a documented marker of the transition.
- Skipped months. Especially later on, when gaps of 60 days or more become common.
- Flow changing. Lighter some months, heavier others.
- All of it at once, in no order. It isn't a dimmer switch. It's a light with a loose wire.
What should be evaluated
- Bleeding that lasts more than 7 days
- Cycles that come more often than every 21 days
- New, recurrent, or persistent bleeding or spotting between periods
- Bleeding after sex
- Soaking through a pad or tampon every hour for two hours running, or passing clots bigger than a quarter
- Any bleeding at all, 12+ months after your last period
Two number systems, and why they don't match
You'll run into different thresholds depending on where you read:
- Mayo Clinic tells patients to contact a clinician for bleeding lasting longer than 7 days or cycles usually fewer than 21 days apart — a patient-facing “call your doctor” trigger, deliberately set a little wider.
- FIGO — the international body that standardized how clinicians classify abnormal uterine bleeding — uses cycle frequency below 24 days and bleeding duration above 8 days — a clinical classification system.
We use the more conservative number every time, because if we're going to be wrong, we're going to be wrong in the direction of you getting seen.
The thing almost nobody tells you: you can still get pregnant
Irregular doesn't mean infertile. Ovulation is unpredictable in perimenopause, not absent. If pregnancy is possible for you, it belongs on the list of things a clinician checks when your bleeding changes — and menopausal hormone therapy is not birth control. If you need contraception, that's a separate conversation, and a good clinician will have both.
Which bleeding patterns mean you shouldn't start with an online clinic
Certain bleeding patterns warrant in-person evaluation before hormone therapy begins, because hormone therapy can change the bleeding pattern a clinician needs to assess. The clearest are: any bleeding 12 or more months after a final period; soaking a pad or tampon hourly for two consecutive hours; bleeding lasting more than seven days; bleeding more often than every 21 days; and bleeding after sex. None of these patterns proves a serious diagnosis. All of them warrant evaluation.
This is the gate. Everything commercial on this page sits behind it, on purpose.
Postmenopausal bleeding is its own category, and ACOG just raised the bar
Postmenopausal bleeding means bleeding 12 or more months after your final period. If that's you, this is the most important paragraph on this page.
About 90% of women diagnosed with endometrial cancer have postmenopausal bleeding. Read that direction carefully — it describes how the cancer usually announces itself. It does not mean 90% of women with postmenopausal bleeding have cancer. Most don't. But it's why this pattern gets its own tier.
And the guidance changed on April 16, 2026.
For years the standard first step was a transvaginal ultrasound (TVUS) — a wand-based scan that measures the thickness of your uterine lining. ACOG replaced it. The Clinical Practice Update, published in Obstetrics & Gynecology by gynecologic oncologist Dr. David Shalowitz, now recommends transvaginal ultrasound and endometrial tissue sampling together as the initial evaluation for most patients with postmenopausal bleeding. DOI: 10.1097/AOG.0000000000006275.
Why the change? Ultrasound alone was missing cancers. ACOG's language is unusually blunt: using endometrial thickness as a triage tool carries “an unacceptably low sensitivity” for malignant and premalignant disease — with reporting putting 5–12% of endometrial cancers going undetected at first presentation when ultrasound is the only tool used.
Ultrasound alone is now reserved for a narrow group: a single episode of bleeding, a fully visualized lining measuring 4 mm or less, no strong risk factors, and no barriers to prompt gynecologic care. ACOG also notes the combination matters especially for Black women, who face disproportionately higher endometrial cancer incidence and mortality.
The evaluation ACOG now recommends for most postmenopausal bleeding has two parts. The second part requires an exam room. A video visit cannot produce a tissue sample — not at any company, at any price.
Which means that for this specific pattern, the honest answer to “which online menopause clinic should I use” is: not yet. Get seen first.
We'd rather tell you that and lose the click.
Why “older than 45” is the line
For bleeding that isn't postmenopausal, the clearest rule in the guidelines is about age. ACOG says endometrial tissue sampling should be performed as a first-line test in patients older than 45 with abnormal uterine bleeding.Not “consider.” Should.
We're being precise about the wording because it matters: ACOG's threshold is older than 45, not “45 and over.” Some sources round it. We don't.
For patients 45 and under, ACOG identifies persistent bleeding, failed medical management, and risk factors for unopposed estrogen exposure — such as obesity or PCOS — as reasons sampling may be indicated. Other conditions that clinicians weigh include type 2 diabetes, tamoxifen use, and Lynch syndrome or a family history of related cancers.
The honest number, honestly framed
In a single-institution study of 1,017 women aged 45 and older who were already undergoing a diagnostic workup for abnormal or postmenopausal bleeding, 5.6% were diagnosed with atypical hyperplasia or endometrial cancer.
That is not your risk. That group was selected — they'd already been referred for a workup, and they were all over 45. We're including it because it's the only peer-reviewed figure that captures the shape of this expense: the workup is not a rounding error, and roughly one in eighteen of the women who go through it turn out to have something that needed finding. Not enough to panic. Far too many for “let's just keep an eye on it” to be the same thing as an answer.
Get evaluated, get your answer, get on with your life.
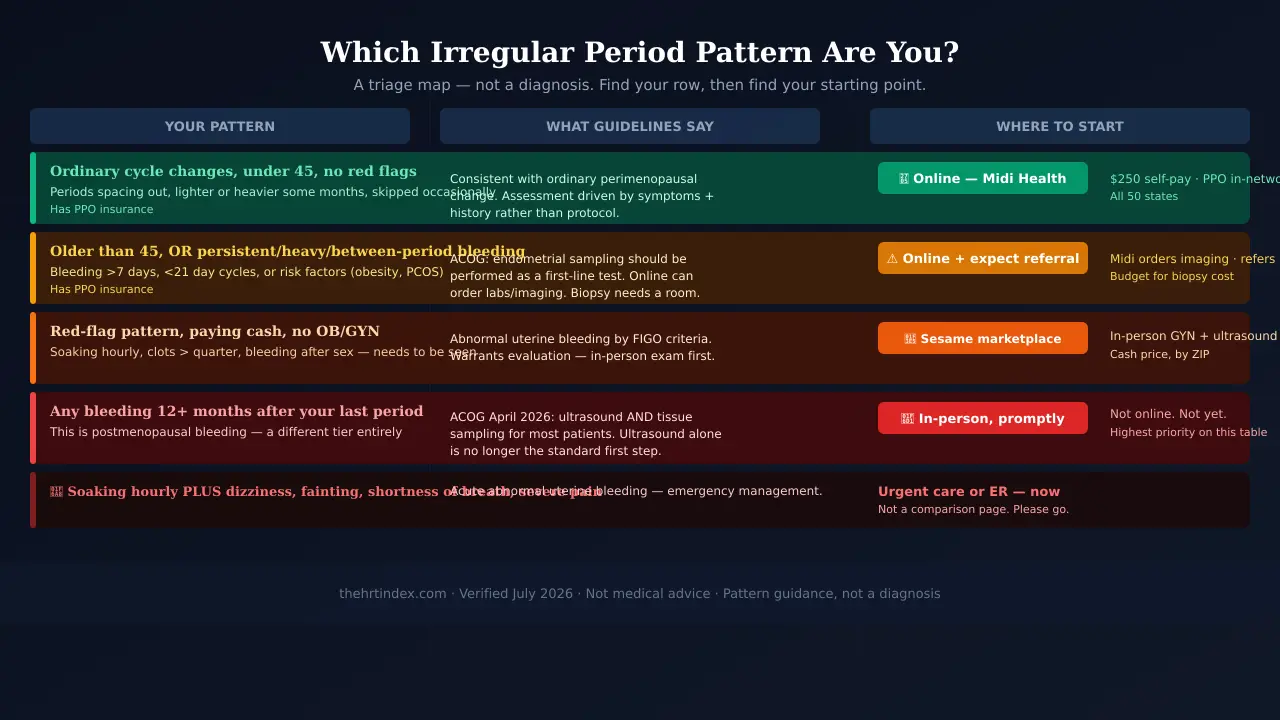
🔬 The Irregular Bleeding Triage Table
What published guidelines say about patterns like yours, and whether an online visit can deliver that evaluation. This is guidance mapping, not a diagnosis. Where a pattern sits near a line, we route it up a tier, not down.
| Your pattern | What guidelines call for | Can an online visit deliver it? | Where to start |
|---|---|---|---|
| Cycle length varying; occasional skipped month; flow changed. Under 45, no risk factors. | Consistent with ordinary perimenopausal change. Assessment driven by symptoms and history. | Yes. History, labs, treatment, follow-up — where the service's model and your state's rules permit. | ✅ Online is a legitimate first stop. |
| Abnormal bleeding, older than 45. | ACOG: endometrial tissue sampling should be performed as a first-line test. | Partly. A clinician can take the history, order labs and imaging, and refer. The tissue sample needs an exam room. | ⚠️ Online can start it — a referral is coming. Budget for it. |
| 45 or under with persistent bleeding, failed treatment, or risk factors (obesity, PCOS, type 2 diabetes, tamoxifen, Lynch syndrome). | ACOG: sampling may be indicated. | Partly. Same as above. | ⚠️ Online can start it — flag your risk factors at intake. |
| Bleeding every ~2 weeks or more often; won't stop after 2+ weeks; soaking hourly for 2+ hours; bleeding after sex; large clots. | Abnormal uterine bleeding by FIGO criteria. Warrants evaluation. | Not as a first step. | 🛑 In-person evaluation first. Don't start hormones before it. |
| ANY bleeding 12+ months after your last period. | ACOG, updated April 16, 2026: transvaginal ultrasound and endometrial tissue sampling together as initial evaluation for most patients. | No. | 🛑 In-person evaluation, promptly. Highest priority on this table. |
| Soaking hourly plus dizziness, fainting, shortness of breath, severe pain, or fever. | Acute abnormal uterine bleeding. | No. | 🚨 Urgent or emergency care now. |
Why we built this: we went looking for one place that joins ACOG's age threshold, ACOG's April 2026 postmenopausal bleeding update, and what a video visit can physically deliver. We couldn't find it. So we assembled the join ourselves, and we'll keep it current.
🟢 Not sure which row is yours?
Most women land between two of them and can't tell which. That's normal — and it's the one question you need answered before you spend a dollar.
Match your bleeding pattern to the right starting point →Free, no email, and it will tell you if online care is the wrong move for you.
What an online menopause clinic can and can't do for irregular bleeding
A virtual menopause clinician can take a full history, order clinically indicated blood work and imaging where the service's model and state rules allow, prescribe medication, and refer out. No video visit can perform an endometrial biopsy or place an IUD, because both are physical procedures. One of those is part of the diagnostic evaluation; the other is a treatment. This is a limitation of the delivery model, not of any single company.
🔴 The two rows that change everything
We built a capability matrix for eight services. Two rows came back identical across every one — and they come back that way for a reason no company can engineer around:
Can a video visit perform an endometrial biopsy? No.
Can a video visit place an IUD? No.
An endometrial biopsy is a tissue sample from your uterine lining, sent to a lab where a pathologist looks at the cells. It takes a few minutes in an office. It's the test ACOG names in both the older-than-45 rule and the April 2026 postmenopausal bleeding update. That one is diagnosis.
A levonorgestrel IUD — Mirena or Liletta — is a small T-shaped device placed inside the uterus that releases progestin locally. FDA-approved for the treatment of heavy menstrual bleeding for up to five years in women who choose intrauterine contraception.
One of the most effective FDA-approved options for the most common version of your complaint is a device that no video visit can give you.
🔴 So here's our damaging admission, and we're putting it before the sales pitch
Midi cannot examine you. No biopsy, no IUD, no hands on your abdomen. If your bleeding pattern needs a room and a speculum before it needs a prescription, Midi is a step in your process, not your process — and Sesame's in-person route is genuinely the better move.
But because Midi isn't running physical clinics, it can offer the thing physical clinics ration hardest: time with a menopause clinician, billed to your insurance. A 30-minute initial visit. Fifteen-minute follow-ups. A clinician who does this all day and can order the imaging when your history calls for it.
For scale: Gennev — a competitor we earn nothing from — cites an average OB/GYN appointment wait of 31.4 days in its own clinician-facing materials. That's Gennev's number, not our measurement, and your market may be faster or slower. But it probably matches what you found when you tried to book one.
🔬 The Capability Matrix
Last verified July 17, 2026. Read from each provider's own published pages and help centers.
✅ Verified— provider says so, or physically inherent to the care model. ❌ No — provider says it doesn't, or physically impossible. —not publicly documented as of July 17, 2026. Silence is not a “no.” Ask before you pay. ⭐ = we may earn a commission.
| Capability | ⭐ Midi | ⭐ Sesame | ⭐ Hers | ⭐ Winona | ⭐ Inner Balance | Gennev | Evernow | Alloy |
|---|---|---|---|---|---|---|---|---|
| Live video visit | ✅ ~30 min | ✅ Subscription incl. video | — Online intake + provider review | ❌ Async only | ❌ No visit required | ✅ 30 min, doctor-led | ✅ Optional | ❌ Async |
| Bills insurance | ✅ Most PPO | ❌ Not for care fees | ❌ | ❌ | ❌ | ✅ | ✅ Video visits | ❌ |
| Medicare/Medicaid | ❌ Neither | ❌ No insurance billing | ❌ | ❌ | ❌ | — | ❌ Neither | ❌ |
| HSA/FSA | ✅ | ✅ Itemized bill on request | — | ✅ By reimbursement | ✅ | — | ✅ | ✅ |
| Can order labs | ✅ | ✅ 5 named labs incl. in subscription | — | Doesn't require any to prescribe | — | — | ✅ Case-by-case | — |
| 🔑 Can order imaging | ✅ “any blood work and/or imaging needed” | ✅ Marketplace lists pelvic ultrasounds, by ZIP | — | — | — | — | — | — |
| 🔑 Endometrial biopsy on a video visit | ❌ | ❌ (marketplace can list an in-person gyn who does) | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ |
| 🔑 IUD placement on a video visit | ❌ | ❌ (marketplace can list an in-person gyn who does) | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ |
| In-person listings | ❌ Refers you out | ✅ By ZIP; availability varies | ❌ | ❌ | ❌ | ❌ | ❌ | ❌ |
| FDA-approved products | ✅ | ✅ incl. estradiol, Prometrium, Bijuva | ✅ | ✅ Tablets, capsules, patches | ❌ | ✅ | ✅ | ✅ Estradiol patch |
| Compounded products | ✅ Yes — Custom Rx | ✅ BHRT if provider deems appropriate | — | ✅ | ✅ Only model | — | — | — |
| States | All 50 (Custom Rx: not all 50) | All 50 | Not all 50 | Not all 50; ages 35–59 | Company says 43 + DC | All states, all ZIPs | — | — |
First: almost every service here now sells compounded hormones — including our top pick. That is new, it is not a scandal, and we explain why it happened. But it means “is this FDA-approved?” is now a product question, never a brand question. Ask about the specific bottle.
Second: Sesame is two different things under one brand. It runs a dedicated menopause subscription (video visits, unlimited messaging, five named labs) and a cash-pay marketplace (book any clinician, including in-person gynecology and ultrasounds, by ZIP). Most reviews describe one and quote the price of the other. We separate them below.
Why “no bloodwork required” is a feature for hot flashes and a problem for bleeding
Winona's own site states it does not require any bloodwork or hormone testing to prescribe. Inner Balance's model states no separate visit and no routine labs are needed to begin.
To be fair to both: these are not no-clinician models. And for a 52-year-old with textbook hot flashes and no bleeding, skipping the hormone panel is defensible — panels genuinely don't tell you much in perimenopause.
For a woman with abnormal bleeding, it's a different story. An online assessment with no scheduled live conversation and no routine testing is a model built for a problem that isn't yours. That objection has nothing to do with formulation. It would stand if every product they shipped were FDA-approved.
🟢 If your bleeding is the ordinary perimenopausal kind, here's the strongest place to start.
Midi runs live 30-minute visits, is available in all 50 states, is in-network with most PPO plans, and its clinicians can order the imaging when your history calls for it.
See if Midi is in-network with your plan →Not on a PPO? Compare the cash-pay routes below before you go anywhere.
The tests your bleeding pattern actually calls for
There is no standard test panel for irregular perimenopausal bleeding. Depending on age, pattern, pregnancy possibility, symptoms, and risk factors, evaluation may include pregnancy testing, a complete blood count, iron or thyroid testing, imaging, and — in some patients — endometrial tissue sampling. Hormone level testing is generally not used to diagnose perimenopause, because levels fluctuate substantially during the transition.
ACOG's patient guidance supports history, physical and pelvic examination, and selective testing — not a fixed six-item bundle for everyone.
| Test | What it's checking | Who publicly documents ordering it |
|---|---|---|
| Pregnancy test | Pregnancy remains possible in perimenopause and changes the whole workup. | Midi ✅ |
| Complete blood count (CBC) | Assesses anemia, which can contribute to fatigue, weakness, dizziness, or breathlessness. | Midi ✅ · Sesame ✅ (named in subscription) |
| Ferritin / iron studies | Iron stores, when iron deficiency is suspected. | Midi ✅ · Sesame: not in the named subscription labs — ask |
| TSH (thyroid) | Thyroid disease can cause menstrual changes and symptoms that overlap with perimenopause. | Midi ✅ · Sesame ✅ (named in subscription) |
| Transvaginal ultrasound | Measures the endometrium; looks for fibroids and polyps. | Midi ✅ (orders it; you go to a local imaging center) · Sesame ✅ (marketplace listing, by ZIP) |
| Endometrial biopsy | Provides tissue for a pathologist to assess. | ❌ No video visit. In-person only. |
The detail worth the whole section: Sesame publishes exactly which labs its menopause subscription includes: CBC, hemoglobin A1c, thyroid function, lipid panel, and a comprehensive metabolic panel. That's an unusually transparent list, and we'd like more companies to publish one.
It's also worth reading closely if you're bleeding. Ferritin and a pregnancy test are not on it. That doesn't mean a Sesame provider can't order them — it means they're not in the included set, so ask what they'd cost.
The one thing Midi and Winona agree on
Worth flagging, because these two companies agree on almost nothing.
Hormone level testing generally can't diagnose perimenopause. Estrogen and FSH swing week to week during the transition, so a single panel tells you little. Both Midi and Winona say so publicly. So does Cleveland Clinic.
Which means: a single normal hormone panel does not rule out perimenopause. If you've been told otherwise, the science is on your side — perimenopause is identified from your age, your cycle history, and your symptoms, not from one blood draw.
Best online menopause clinic for irregular periods, by your situation
There is no single best online menopause clinic for irregular periods — there is a best starting point for your bleeding pattern, your state, and how you're paying. For ordinary perimenopausal change with PPO insurance, Midi Health. For a pattern that needs an in-person exam without insurance, Sesame's marketplace. For cash-pay FDA-approved hormones after evaluation, Hers or Alloy. Neither Midi nor most of this category accepts Medicare or Medicaid.
| If you are… | Start with | Why | What it won't do |
|---|---|---|---|
| Under 45, ordinary cycle changes, PPO insurance | Midi Health | Insurance, live 30-min video, all 50 states | Won't examine you |
| Older than 45, abnormal bleeding, PPO insurance | Midi Health — expect a referral | Can order imaging; refers with after-visit summary | Won't do the biopsy |
| Any red-flag pattern, need to be seen | In-person first. Sesame's marketplace if paying cash | Only route that lists in-person gyn and ultrasounds by ZIP | Listings vary by location |
| Postmenopausal bleeding (12+ months, then bleeding) | In-person, promptly | ACOG April 2026: ultrasound and sampling for most patients | Not online. Not yet. |
| Want a doctor-led video visit, nationwide | Gennev (we earn nothing) | Board-certified OB/GYNs, 30-min visits, all states, takes insurance | Imaging workflow isn't publicly documented |
| Evaluated, cash-pay, price-sensitive | Compare Hers and Alloy | Both publish FDA-approved prices; Alloy estradiol patch from $74.99/mo, Hers oral from $79/mo | Neither bills insurance; check your state |
| On Medicare or Medicaid | Not this category | See below | — |
| Post-hysterectomy (no uterus) | Different page → | No endometrium changes the calculation | — |
If you have Medicare or Medicaid
We're going to lose the click here and publish it anyway.
Midi is not enrolled with Medicaid or Medi-Cal and states it cannot treat those patients at this time — even as self-pay. Midi is not covered by Medicare either; it can accept Medicare beneficiaries as self-pay patients, but no claims can be submitted for visits, medications, or related services. Evernow states it does not support Medicare or Medicaid coverage. Sesame, Hers, Winona, Inner Balance, and Alloy don't bill insurance at all. Gennev's current Medicare and Medicaid position isn't stated in the public materials we reviewed — ask them directly rather than take our silence for a no.
So if you're on Medicare or Medicaid, this category is mostly built for someone else. What we'd do instead:
- Use The Menopause Society's “Find a Menopause Practitioner” directory to locate an MSCP-credentialed clinician who takes your coverage. It's free, and MSCP is the real external credential in this field.
- Ask your primary care clinician for a gynecology referral. Describe your actual pattern — how many days, how heavy, how often, and any bleeding between periods or after sex. Specific beats vague, every time.
- Bring your cycle dates written down. Six months of them, with duration and flow. It's the most useful thing you can hand a clinician.
Midi Health for irregular periods: what it does, what it costs, what it can't do
Midi Health is a virtual perimenopause and menopause clinic available in all 50 states, with 30-minute initial video visits and 15-minute follow-ups. It is in-network with most PPO plans; self-pay is $250 for an initial visit and $150 for continued care. Its clinicians can order clinically indicated blood work and imaging, and prescribe both FDA-approved and compounded hormone therapies. It does not accept Medicare or Medicaid and does not provide in-person care.
One sentence makes Midi the answer for this query, and it's Midi's own:
“Midi orders any blood work and/or imaging needed… and we refer you to your regular doctors or specialists for any necessary in-person care.”
Not just labs. Imaging. Nobody else in the affiliate space publishes that sentence, and imaging is the exact capability the gap between “ordinary perimenopause” and “needs a closer look” runs through.
| What we verified about Midi | |
|---|---|
| Visit format | Live video. ~30 min initial, ~15 min follow-up |
| States | All 50 for care. Custom Rx compounded products: not all 50 |
| Insurance | In-network with most PPO plans. Coverage varies by plan; deductibles, coinsurance, and copays still apply |
| Self-pay | $250 initial · $150 continued care |
| Medicare | Not covered. Self-pay only; no claims submitted |
| Medicaid / Medi-Cal | Not enrolled. Cannot treat these patients, even self-pay |
| HSA/FSA | Yes, for copays and services |
| Labs & imaging | Orders both; completed at local labs and imaging centers |
| Medications | FDA-approved therapies and compounded options via Midi Custom Rx |
| In-person care | None. Refers to your own doctors and specialists |
| Accreditation | Midi displays an NCQA accreditation seal and LegitScript certification on its site |
The part we have to tell you about our own top pick
Midi now sells compounded hormones. Its own site says so: “Midi also now offers compounded HRT options with both estrogen and progesterone therapies.” They're sold through Midi Custom Rx — estradiol gel from $60, estradiol cream from $45, and progesterone capsules from $35 per 30-day supply. Midi's own disclaimer states: “Compounded drugs are not FDA-approved. The FDA has not verified the safety, effectiveness, or quality of this product.”
Why does this exist? Because there's a shortage: certain hormone therapy medications — including estrogen patches, some oral estrogen, and oral progesterone — are in short supply at pharmacies in parts of the US. Compounding is one way clinics are keeping patients on treatment.
We're telling you because it changes what you ask for. “Is Midi FDA-approved?” is not a question with an answer. Midi is a clinic. It prescribes both categories. The FDA-approved question belongs to the bottle, not the brand — and on this page, with your bleeding, it belongs on the FDA-approved side. Ask for it by name.
About the clinicians — one distinction worth knowing
Midi's clinicians include nurse practitioners, certified nurse-midwives, physicians, and naturopathic doctors, trained internally through a program Midi calls Midi University. That's real. It's also not the same thing as the Menopause Society Certified Practitioner (MSCP) credential, which is an external certification from The Menopause Society. Both exist. They're different. A company's internal training program is a company's internal training program.
If MSCP specifically matters to you, ask, or use The Menopause Society directory.
What Midi's own patients say
These are testimonials Midi selected and published on its own website. We confirmed they appear there on July 17, 2026. We did not independently verify the patients or test appointment availability. We include them because they describe scheduling and being listened to — the part a company's testimonial page can honestly speak to.
“Midi was so easy: I got a same day appointment and they took my insurance.” — Victoria W.
“I spent almost three years being dismissed by doctors, and told to nap more.” — Libby H.
🟢 Thirty minutes with a clinician who does this all day.
That's the appointment your last one wasn't. Checking coverage doesn't book you, charge you, or commit you to hormones.
See if Midi is in-network with your plan →If you need to be seen in person: Sesame
Sesame is a cash-pay healthcare marketplace that also runs a dedicated menopause subscription. The subscription includes video visits, unlimited messaging, and five named lab tests if ordered. The marketplace lists individual clinicians at upfront prices, including in-person gynecology and pelvic ultrasounds, with availability varying by location. Sesame does not bill insurance for care fees.
If the triage table put you in the red-flag rows, this is your section. Everything above was setup.
1. The menopause subscription
Ongoing care: a video visit with a provider you choose, unlimited messaging, same-day prescriptions to your local pharmacy, and basic lab work if your provider orders it. A real ongoing program, not a one-off appointment.
2. The marketplace — for red-flag rows
Book any of Sesame's clinicians directly, at their own upfront cash price, across 36+ specialties in all 50 states — including in-person gynecology and pelvic ultrasounds, which Sesame advertises at up to 60% off typical rates. This is the one you want if you're in the red-flag rows.
Good, and genuinely unusual:
- The included labs are named. CBC, hemoglobin A1c, thyroid function, lipid panel, comprehensive metabolic panel — published, per state.
- The refund policy is published. Cancel at least 3 hours before your initial visit for a full refund.
- HSA/FSA works. Sesame will send an itemized bill on request.
- They tell the truth about compounded. Sesame's own FAQ states that BHRT “is prescribed and dispensed outside of formal FDA regulation” — a more honest disclosure than most of this industry manages.
The catches, and they're real:
- No insurance billing for care. If you have a good PPO, your copay may beat Sesame's cash price.
- You're choosing a person, not a brand standard. Quality varies by clinician. Read the profile.
- No controlled substances online. That matters if testosterone comes up.
- Medication isn't included in the subscription price.
- The price question has two answers, and one disagrees with itself. Official Sesame surfaces have shown $54 on one and $59 on another. Verify at live checkout.
🟢 If your pattern is on the red-flag list, the evaluation comes before the treatment.
Not because something is wrong. Because starting hormones first makes the picture harder to read — and the fastest way to stop worrying is to find out.
Check in-person gynecology and ultrasound listings near you →You'll see the real price before you book. Listings and prices vary by ZIP and clinician.
Cash-pay FDA-approved hormones: Hers and Alloy
Hers publishes FDA-approved menopause therapy from $79 per month for oral treatment and $134 per month for patches on 12-month plans. Alloy publicly lists an FDA-approved estradiol patch from $74.99 per month. Neither bills insurance, and neither publicly documents live video visits or imaging orders for irregular bleeding. Both suit women whose bleeding has already been evaluated.
Short section, because these two have a narrow but real job here: cash-pay access to FDA-approved hormones once you know what you're treating.
What we like about Hers: it's transparent about something the rest of this category buries. Hers' own site notes that hormone therapy is not FDA-approved specifically for perimenopause and is prescribed off-label at a clinician's discretion. Individual FDA-approved menopausal hormone products carry specific labeled indications — hot flashes and night sweats, vulvovaginal symptoms, prevention of osteoporosis. Regulating an irregular cycle is not among them. Off-label prescribing is legal, common, and often appropriate. But if a provider implies HRT is the FDA-approved fix for your irregular periods, that provider is telling you something that isn't true.
The honest limits on both: no insurance billing, not every state, and neither publicly documents a live-video visit or an imaging-order workflow for irregular bleeding. That's an evidence gap, not a denial — but if you haven't been evaluated yet, start somewhere that documents ordering tests. Come back here after.
What this actually costs — including the tests nobody quotes
The consultation is the small number. Cash prices for a transvaginal ultrasound vary widely by market and facility. In a single-institution study of women undergoing a diagnostic workup for abnormal or postmenopausal bleeding between 2013 and 2017, median 90-day health-system cost was $2,279 in inflation-adjusted 2017 dollars. Comparison pages quote the monthly subscription; the evaluation is the expense that determines the budget.
You came in budgeting $99 a month for a cream. Let's do the real math — carefully, because this is where most pages start making numbers up.
| Step | What we can actually tell you | Who can order it |
|---|---|---|
| Online menopause consult | Midi: $250 initial, $150 continued care — published. Gennev: $250 initial, $199 follow-up — published. Evernow: $150 self-pay video visit; membership $49/mo, $129/3 mo, or $420/yr. Alloy: $49 consult. Sesame: verify at live checkout. | — |
| Blood work | Depends entirely on your plan and lab. Sesame includes five named labs in its subscription if ordered — the most concrete answer any provider here gives. Midi orders them; you pay your lab. | Midi ✅ Sesame ✅ |
| Transvaginal ultrasound | Varies widely by market and facility. One observed cash-pay listing: from approximately $211 via MDsave. Sesame advertises marketplace pelvic ultrasounds at up to 60% off typical rates. Hospital-based imaging typically costs more than an outpatient imaging center. Get a written cash price for your ZIP before you book. | Midi ✅ Sesame ✅ |
| Endometrial biopsy | Priced by the performing practice. Generally covered by insurance when medically indicated. | ❌ No video visit. In-person only. |
| The whole workup, for scale | In a single-institution cohort of 1,017 women aged 45 and older worked up for abnormal or postmenopausal bleeding 2013–2017: median 90-day health-system cost $2,279 (IQR $512–$4,828), inflation-adjusted 2017 dollars. Benign result: median $2,203. Endometrial cancer diagnosis: median $21,039. This is not your cash bill and not your out-of-pocket. We're including it because it captures the shape of this expense. | — |
Where insurance earns its keep: not on the consult. On the imaging and the biopsy. That's the argument for Midi's PPO network over a cheaper subscription — if you have a PPO. If you don't, Sesame's upfront cash listings are the honest alternative.
What happened when we tried to price all eight
Price transparency is one of the five pillars of The HRT Index Verification Standard. We don't just record the price — we record how hard it was to find. That turns out to be information about the company.
| Service | Price on their own site? | What we found |
|---|---|---|
| Midi Health | ✅ Plainly | $250 / $150 on a dedicated pricing page, with Medicare and Medicaid exclusions in the same paragraph. The most transparent disclosure in this group. |
| Gennev | ✅ Plainly | $250 initial doctor visit, $199 follow-up; 30-minute visits; video in every state. We earn nothing from Gennev. |
| Hers | ✅ Yes | $79/mo oral, $134/mo patch on 12-month plans |
| Alloy | ✅ Yes | Estradiol patch from $74.99/mo; $49 consult |
| Evernow | ⚠️ Yes, but read the asterisk | $49 month-to-month, $129/3 months, $420/year. The “$35/month” you'll see quoted is the annual plan's monthly equivalent, not a monthly price. Self-pay video visits are $150. |
| Sesame | ⚠️ Two models, one disagreement | Marketplace visits are priced per clinician — no single number exists, by design. For the subscription, official surfaces have shown $54 on one and $59 on another. Verify at live checkout. |
| Winona | ⚠️ Per product | Priced by product, not by care. There's no consult fee to compare because there's no scheduled consult — it's async intake with clinician review. |
| Inner Balance | ⚠️ Partial | Public Oestra materials display pricing from $99.50/month; reviewed program terms showed $199/month for the first six months, then $99.50. Capture the current checkout before relying on either. |
What actually treats irregular perimenopausal bleeding
Options for abnormal perimenopausal bleeding after evaluation include a 52 mg levonorgestrel IUD (FDA-approved for heavy menstrual bleeding for up to five years in women who choose intrauterine contraception), combined hormonal contraception, cyclic or continuous progestogens, and tranexamic acid (FDA-approved and non-hormonal). Menopausal hormone therapy is not FDA-approved to regulate menstrual bleeding and does not replace evaluation of unexplained abnormal bleeding.
HRT is not FDA-approved to regulate your cycle.
Individual FDA-approved menopausal hormone products carry specific labeled indications — hot flashes and night sweats, vulvovaginal symptoms, prevention of osteoporosis. None of them says “makes your periods regular.” The FDA also advises women with vaginal bleeding problems to discuss them with a healthcare professional before starting hormone therapy.
Different hormonal regimens do affect bleeding, and clinician-directed hormone treatment can absolutely be part of an overall plan once you know what you're treating. But “I have bleeding changes” and “I have hot flashes” are two goals needing two conversations. A provider who collapses them into one is selling, not treating.
1. The levonorgestrel IUD (Mirena, Liletta)
A small device placed in the uterus that releases progestin locally. FDA-approved for the treatment of heavy menstrual bleeding for up to five years in women who choose intrauterine contraception. It thins the lining, which is why it works, and it handles contraception, which you may still need.
It requires an in-person procedure. No video visit can place it.
2. Combined hormonal contraception
The pill, patch, or ring. Often first-line for the irregular anovulatory bleeding of perimenopause, because it takes over the cycle rather than negotiating with it. Also handles contraception. Prescribable online.
3. Cyclic or continuous progestogens
Including FDA-approved micronized progesterone. Gives the lining the “stop and shed” signal your ovary isn't sending. Prescribable online.
4. Tranexamic acid (Lysteda) — the one nobody mentions
Non-hormonal. FDA-approved for cyclic heavy menstrual bleeding in females of reproductive potential. You take it only on your heavy days. It slows the breakdown of clots, reducing bleeding without touching your hormones.
- Its labeling directs clinicians to exclude endometrial pathology associated with heavy bleeding before prescribing.
- It is contraindicated with combined hormonal contraception — options 2 and 4 are not a combination you stack.
- It is contraindicated in patients with active, prior, or intrinsic risk of thrombosis.
If you've read this far thinking “I don't want hormones” — this is the option most menopause listicles leave out. Ask about it by name.
Why we don't recommend compounded hormones on this page
Compounded hormone products are custom-mixed by pharmacies for individual patients. They are not FDA-approved, and the FDA does not review them for safety, effectiveness, or quality before marketing. For irregular perimenopausal bleeding, the clinical objective is protecting the endometrium — the specific area where major reviews including NASEM and ACOG have found the available evidence on compounded regimens inadequate.
We earn a commission from Winona and Inner Balance. Winona is our highest-paying partner.
We're telling you not to use either of them for this.
Here's the reasoning, so you can check it instead of taking our word.
What “compounded” means, precisely
A compounded drug is mixed by a pharmacy to a prescriber's specification for an individual patient. It's legal. Real clinicians prescribe it. It has genuine uses — an allergy to a dye, a dose that isn't manufactured, a form you can't swallow. The FDA's position is that compounded drugs are appropriate for patients whose medical needs cannot be met by an FDA-approved drug.
But: compounded drugs are not FDA-approved. The FDA does not review them for safety, effectiveness, or quality before marketing. That's not an insult. It's the regulatory definition, and Midi, Sesame, and Winona all print versions of it on their own sites.
Why 2026 made this suddenly urgent
There's a shortage. Certain hormone therapy medications — including estrogen patches, some oral estrogen, and oral progesterone — are in short supply at pharmacies across parts of the US. Compounding is one of the ways clinics are keeping women on treatment through it.
So the honest version of the 2026 landscape isn't “compounded brands versus real ones.” It's that nearly every service on this page now sells both — Midi included. The question you ask has to change: not “is this company legit?” but “is this specific bottle FDA-approved, and if not, why not?”
Why it matters specifically for your bleeding
Go back to the mechanism. Your bleeding is irregular because ovulation is unreliable, so estrogen builds your lining with no progesterone to end the cycle. The clinical problem is endometrial protection.
That's precisely where the evidence on compounded regimens is thin:
- NASEM (2020): low-dose progesterone has not been found to protect the endometrium and reduce the endometrial cancer risk induced by unopposed estrogen.
- ACOG Clinical Consensus (2023): data on compounded bioidentical hormone therapy are minimal and assess only surrogate markers; data were inadequate to assess endometrial cancer risk.
- The Menopause Society: compounded bioidentical hormones are not recommended for menopause symptoms.
- British Menopause Society (May 2026): absorption of compounded transdermal progesterone is variable, and it may not provide sufficient endometrial protection.
To be precise: major reviews found insufficient evidence to establish reliable endometrial protection for the compounded regimens they evaluated. “We don't know” is a different answer than “it's fine,” which is how it's usually sold.
🎯 And then the FDA did something that made this unmissable
On February 12, 2026, the FDA approved labeling changes for six menopausal hormone therapy products, removing boxed-warning risk statements about cardiovascular disease, breast cancer, and probable dementia.
One warning stayed.
The FDA stated it was “not seeking to remove the boxed warning for endometrial cancer for systemic estrogen-alone products.” If you have a uterus and you take estrogen, you need a progestogen. That one didn't move an inch.
Out of everything the FDA reconsidered and relaxed, the one thing it declined to touch is the exact thing your bleeding is about.
And the care model, separately from the formulation
Winona operates asynchronously with no live video and states it doesn't require any bloodwork or hormone testing to prescribe. Inner Balance's Oestra is a compounded estradiol and progesterone vaginal cream, ordered through an online questionnaire with licensed-clinician review and no separate scheduled visit or routine labs to begin.
Both have a prescriber. Neither has a scheduled live conversation. For a woman with abnormal bleeding, an online assessment with no live discussion and no routine testing is a model built for a different problem.
One thing we could not resolve: Inner Balance's own public materials conflict on whether its compounding model is 503A (a pharmacy compounding for individual patients) or 503B (a registered outsourcing facility with different federal oversight). Both appear across its pages. Confirm it directly before you buy.
Where these providers legitimately fit
We're not saying nobody should use them. We're saying not you, not for this, not yet:
- After a total hysterectomy. No uterus, no endometrium — the endometrial-protection objection genuinely changes. But it doesn't erase the rest: the product's FDA status, quality oversight, dosing consistency, and evidence base are all still what they were. → HRT after hysterectomy
- When a licensed clinician identifies a patient-specific medical need that an available FDA-approved product can't meet — which is the standard the FDA actually names for compounding. That's a real conversation with a real prescriber, not a checkout preference.
Why we're telling you this
Because an affiliate site that only ever recommends what pays it isn't a comparison. It's a catalog with a search box.
The point of having a verification standard is that it sometimes returns an answer we don't like. This is one of those. We'd rather you check us than trust us — every claim above has a citation, and they all lead somewhere you can read yourself.
No CTA in this section. On purpose. A button here would prove we didn't mean it.
What to ask before you pay
Before paying an online menopause clinic when irregular bleeding is the reason for the visit, confirm the visit format, whether the clinician can order imaging, what happens if you need a biopsy, whether the specific medication offered is FDA-approved or compounded, the total cost including labs, and the cancellation terms.
Copy these. Ask them in the chat window before you pay. Three minutes, and you won't waste a consult.
- 1. Will my first visit be live video, or is this messaging only? (If they won't say, it's messaging.)
- 2. Can the clinician order pelvic or transvaginal imaging if my history calls for it? (The highest-value question on this list.)
- 3. What happens if I need an endometrial biopsy — do you refer, and do you send my records to whoever does it?
- 4. Is the specific medication you'd prescribe me FDA-approved or compounded? (Ask it exactly like that. It's about the bottle rather than the brand, and in 2026 you cannot guess it from the logo.)
- 5. What's the total for the visit, follow-up, labs, and medication — before I book?
- 6. How do I cancel, and what's the refund window?
How we verified this
The HRT Index Verification Standard: we read every published price, separate FDA-approved from compounded, verify state availability and insurance, and re-check on a fixed schedule — top providers monthly, full roster quarterly. It is not a numeric score and we do not assign per-provider ratings. This page was verified on July 17, 2026.
✅ What we verified — July 17, 2026
Checked against providers' own public materials: Insurance status and network language · state availability · visit format · lab and imaging ordering language · FDA-approved vs. compounded product categories · published pricing · stated clinician credentials · included lab lists · refund terms · testimonial text and placement
Traced to primary sources: ACOG's abnormal uterine bleeding guidance and its older-than-45 sampling threshold · ACOG's updated postmenopausal bleeding guidance, April 16, 2026, Obstetrics & Gynecology, DOI 10.1097/AOG.0000000000006275 · FDA labeling actions (November 2025 initiation; February 12, 2026 approval) · NASEM 2020 compounded bioidentical hormone report · ACOG Compounded Bioidentical Menopausal Hormone Therapy Clinical Consensus 2023 · Mirena prescribing information · Lysteda prescribing information · peer-reviewed AUB workup cost data (n=1,017)
⚠️ What we could NOT verify
Inner Balance's 503A vs. 503B designation — its own pages conflict, and we did not choose one · Inner Balance's state count (company-published) · Gennev's Medicare and Medicaid position · Sesame's live subscription checkout price (official surfaces disagree) · imaging-order workflows at Hers, Winona, Inner Balance, Gennev, Evernow, and Alloy (not documented publicly — which is not the same as “no”) · HSA/FSA specifics for Hers · ZIP-level in-person and imaging availability on Sesame's marketplace
❌ What we did NOT do
We did not sign up as patients. We did not time support responses, test appointment availability, complete a checkout, test cancellation, or receive care from any provider. We are not claiming firsthand testing we didn't do. Where we quote a provider's own claim about speed or convenience, we attribute it to them rather than adopt it. No provider reviewed this page before publication, and none paid for placement, for copy, or for a conclusion.
The five pillars, applied to this specific question
We evaluate every provider on exactly five things, always in this order. Here's what each meant for irregular bleeding.
- 1. Clinical legitimacy. Licensed clinicians, appropriate scope, real prescribing requirements, honest safety exclusions. Here: does the model require a clinical assessment before hormones ship?
- 2. Care quality. Live versus async, visit length, continuity, follow-up — and the one that decided this page: does the service publicly document ordering the test and handing off when telehealth isn't enough?
- 3. Medication fit. FDA-approved and compounded, labeled separately, never blurred — product by product, because in 2026 no company here is one or the other. Here: the fit question is endometrial protection, which is where the categories separate hardest.
- 4. Price transparency. Consult, follow-up, membership, medication, labs, cancellation — and whether you can see any of it before an intake. We logged it.
- 5. Access. States, insurance, Medicare, Medicaid, format, eligibility limits. Here: the Medicare and Medicaid answer is no or unstated across the board, and we published that even though it costs us the click.
Frequently asked questions
Are irregular periods normal during perimenopause?
Cycle changes are the defining feature of perimenopause — one frequently cited distribution found only about 12% of women stop menstruating suddenly with no irregular bleeding at all. But 'common' is not 'no need to look.' Bleeding longer than 7 days, more often than every 21 days, after sex, or 12 or more months after your last period should be evaluated rather than assumed.
When should I worry about irregular periods in perimenopause?
'Worry' isn't the right frame — 'get it checked' is. Contact a clinician if you're soaking a pad or tampon hourly for two hours, bleeding longer than seven days, bleeding more often than every 21 days, bleeding between periods or after sex, or bleeding at all 12 or more months after your last period. None of these proves something is wrong. All of them warrant evaluation.
Can an online menopause clinic perform an endometrial biopsy?
No. An endometrial biopsy is a physical procedure performed in an exam room — a video visit cannot produce a tissue sample, at any company, at any price. A virtual clinician can take the history, order clinically indicated tests where its model allows, and refer you to someone who performs the biopsy. Some platforms, like Sesame's marketplace, list in-person gynecology separately, but that's a different appointment you book yourself.
Can an online doctor treat irregular periods?
Partly. A virtual clinician can take a full history, order clinically indicated blood work and imaging where the service's model and state rules permit, prescribe medication, and refer out. No video visit can perform a biopsy or place an IUD. For ordinary perimenopausal change, online care is a legitimate first stop. For red-flag patterns, it isn't.
Will an online menopause clinic make me get an ultrasound?
They can order one if your age, pattern, or risk factors call for it — Midi publicly states its clinicians order any blood work and imaging needed, completed at your local labs and imaging centers. You'd go to a local facility for the scan. Nobody can force you; a clinician can decline to prescribe without it, which is the system working.
Will insurance cover the ultrasound or biopsy ordered after an online visit?
It depends on your plan, the ordering clinician's network status, the facility you use, and your plan's medical-necessity rules — the online visit and the test are billed separately, so one being covered tells you nothing about the other. Ask two questions before you book: is the ordering clinician in-network, and is the imaging facility in-network? An in-network visit that sends you to an out-of-network imaging center is a common and expensive surprise.
What does a transvaginal ultrasound cost without insurance?
It varies widely by market and facility, so treat any single national number with suspicion. One observed cash-pay listing was approximately $211 via MDsave. Sesame advertises marketplace pelvic ultrasounds at up to 60% off typical rates. Hospital-based imaging generally costs more than a standalone imaging center. Get a written cash price for your ZIP before booking.
I'm 43 — am I too young for perimenopause?
No. Perimenopause commonly begins in the forties and can start in the late thirties. 'Too young' is one of the most common things women in this position are told, and it's frequently wrong. Perimenopause is identified from your age, your cycle history, and your symptoms — not from a hormone panel, which fluctuates too much to settle it.
Do online menopause clinics take insurance?
Some do. Midi is available in all 50 states and in-network with most PPO plans; coverage varies by plan and deductibles, coinsurance, and copays still apply. Gennev accepts insurance, and Evernow bills commercial insurance for video visits. Sesame, Hers, Winona, Inner Balance, and Alloy don't bill insurance for care. 'Takes insurance' never means 'your visit is covered' — check your specific plan.
Can I use Medicare or Medicaid?
Not with these. Midi is not covered by Medicare (it can see beneficiaries as self-pay, but no claims can be submitted) and is not enrolled with Medicaid or Medi-Cal — it states it cannot treat those patients at all. Evernow says it doesn't support either. The rest don't bill insurance. Gennev's position isn't stated publicly.
What if I've gone a year without a period and now I'm bleeding?
That's postmenopausal bleeding, and it's the highest-priority pattern here. See a clinician in person, promptly. As of April 16, 2026, ACOG recommends transvaginal ultrasound and endometrial tissue sampling together as the initial evaluation for most patients — a change from the previous ultrasound-first approach. Most causes turn out to be benign. It still needs checking, and it can't be checked online.
Will they just put me on birth control?
Maybe, and it may be the right call. Combined hormonal contraception is often first-line for the irregular anovulatory bleeding of perimenopause — it takes over the cycle instead of negotiating with it, and it handles contraception, which you may still need. It isn't a brush-off. If it feels like one, ask why it was chosen and what the alternatives are.
Can I get an IUD through an online menopause clinic?
No — placement requires an in-person procedure. This matters more than it sounds: the 52 mg levonorgestrel IUD is FDA-approved to treat heavy menstrual bleeding for up to five years in women who choose intrauterine contraception. For some patients with heavy bleeding it's a strong option, and no telehealth service on this page can provide it.
Do I need hormone testing to diagnose perimenopause?
Usually not. Levels swing so much during the transition that a single panel can't confirm or rule it out. Midi and Winona both say so publicly. Selective testing — thyroid, blood count, iron, pregnancy — checks for other causes, which is a different thing from testing 'for perimenopause.'
Can I still get pregnant with irregular periods?
Yes. Ovulation is unpredictable in perimenopause, not absent. Pregnancy stays on the list of things to check when bleeding changes, and menopausal hormone therapy is not contraception. If you need birth control, that's a separate conversation to have on purpose.
Is compounded HRT safe for irregular bleeding?
We won't recommend it for this. Compounded drugs are not FDA-approved and aren't reviewed by the FDA for safety, effectiveness, or quality before marketing. For irregular bleeding the clinical question is protecting the uterine lining — and NASEM reports low-dose progesterone has not been found to protect the endometrium, while ACOG's 2023 consensus found the data inadequate to assess endometrial cancer risk. Note that most services here now offer compounded options, including Midi — so ask about the specific product.
What if I don't want hormones at all?
Ask about tranexamic acid by name. It's non-hormonal and FDA-approved for cyclic heavy menstrual bleeding, taken only on heavy days. Its label directs clinicians to exclude endometrial pathology first, and it's contraindicated with combined hormonal contraception and with thrombotic risk — so it needs a real conversation. It's left out of nearly every menopause listicle because it isn't a hormone. You're allowed to ask for it.
Still not sure which HRT program is right for you?
You now know more about your own bleeding than most women get told in a fifteen-minute appointment. Here's the last mile.
The HRT Index's Find My HRT Path tool matches your symptoms, your age and uterus status, your bleeding pattern, your medication route preference, your insurance or cash-pay situation, and your state to the right provider — and flags when online care isn't the right starting point. No email required. Your answers aren't stored or sent to any provider.
Get my personalized HRT action plan →Sources
1. ACOG. Practice Bulletin 128: Diagnosis of Abnormal Uterine Bleeding in Reproductive-Aged Women. Obstet Gynecol. 2012;120:197–206 — endometrial sampling as a first-line test in patients older than 45 with AUB.
2. Perimenopausal bleeding-pattern distribution (~70% scanty/infrequent, ~18% heavy/excessive, ~12% sudden cessation). PMC9490892
2m. Midi Health. HRT Shortage: How Midi Can Help. joinmidi.com/estrogen-shortage — compounded HRT options; Midi Custom Rx pricing; availability disclaimer. Verified July 17, 2026.
3. Perimenopausal abnormal uterine bleeding. Contemporary OB/GYN — additional risk factors in sampling decisions.
4. Munro MG, et al. FIGO PALM-COEIN classification and standardized AUB definitions. Int J Gynaecol Obstet. 2011;113(1):3–13; FIGO 2018 revision — cycle frequency <24 days, duration >8 days.
6. ACOG. Updated Guidance Regarding the Role of Transvaginal Ultrasonography in Evaluating the Endometrium of Individuals With Postmenopausal Bleeding. Clinical Practice Update. Obstet Gynecol. April 16, 2026. DOI: 10.1097/AOG.0000000000006275. journals.lww.com
7. Mayo Clinic. Perimenopause — Symptoms & Causes. mayoclinic.org — patient-facing contact triggers.
7a. ACOG. ACOG Publishes Updated Guidance on Evaluation of Postmenopausal Bleeding. News release, April 16, 2026. acog.org
8. Healio. ACOG updates guidance for evaluating postmenopausal bleeding. April 22, 2026. healio.com
8m. Midi Health. How Midi Works. joinmidi.com/how-midi-works
9. Contemporary OB/GYN. Clinical pearls into ACOG's postmenopausal bleeding guidelines. June 4, 2026. contemporaryobgyn.net
9a. ACOG. Abnormal Uterine Bleeding (patient FAQ). acog.org
10. Cleveland Clinic ConsultQD. New Guidance Supports Dual Assessment Methods for Postmenopausal Bleeding. 2026. consultqd.clevelandclinic.org
10p. Hers. Menopause. forhers.com/menopause — product page verified July 17, 2026.
11. Inner Balance. Oestra product page; HRT treatment pages. innerbalance.com — compounded estradiol/progesterone vaginal cream; pricing from $99.50/month; 503A and 503B statements conflict across the company's public pages.
11a. Lysteda (tranexamic acid) Prescribing Information. accessdata.fda.gov — indicated for cyclic heavy menstrual bleeding; exclude endometrial pathology before prescribing; contraindicated with combined hormonal contraception and thrombotic risk.
12. Midi Health. Pricing & Insurance. joinmidi.com/pricing-insurance — $250 initial / $150 continued-care; in-network with most PPO plans; not enrolled with Medicaid/Medi-Cal; not covered by Medicare; HSA/FSA accepted; NCQA accreditation. Verified July 17, 2026.
13. Winona. FAQ and product pages. bywinona.com/faq — asynchronous intake; no bloodwork or hormone testing required to prescribe; no insurance billing; ages 35–59; FDA-approved and compounded products listed separately.
13g. Gennev. Insurance & Pricing. gennev.com — $250 initial, $199 follow-up; insurance accepted; video appointments in every state. Non-affiliate.
15. Midi Health. Help center — “Midi orders any blood work and/or imaging needed.” joinmidi.com
15s. Sesame. Menopause subscription terms. sesamecare.com — included labs; refund policy; compounded disclosure; HSA/FSA; no controlled substances online.
16a. Alloy. Product pricing. alloy.com — estradiol patch from $74.99/mo; $49 consult.
17. Sesame. Marketplace. sesamecare.com — in-person gynecology and pelvic ultrasounds by ZIP; up to 60% off typical rates advertised.
17b. Sesame. All 50 states availability. sesamecare.com
18. Hers. Menopause product pages — forhers.com/menopause — FDA-approved from $79/mo oral, $134/mo patch on 12-month plans; off-label prescribing disclosure. Verified July 17, 2026.
21. Evernow. Pricing and terms. evernow.com — $49/mo month-to-month; $150 self-pay video visit; no Medicare or Medicaid.
22. Alloy. Pricing and terms. alloy.com — async; $49 consult; HSA/FSA.
23. Mirena (levonorgestrel-releasing intrauterine system) Prescribing Information — FDA-approved for the treatment of heavy menstrual bleeding for up to 5 years in women who choose intrauterine contraception. accessdata.fda.gov
24f. FDA. Compounding and the FDA: Questions and Answers. fda.gov
25. Cleveland Clinic. Perimenopause. my.clevelandclinic.org — perimenopause begins in forties; hormone levels fluctuate.
26f. FDA. Menopause & Hormones: Common Questions. fda.gov — approved indications; undiagnosed vaginal bleeding as contraindication.
29. MDsave. Transvaginal ultrasound cash-pay listings. mdsave.com — observed price from approximately $211.
31. Peer-reviewed single-institution cohort: 1,017 women aged 45+, 2013–2017 diagnostic workup for abnormal or postmenopausal bleeding; 5.6% atypical hyperplasia or endometrial cancer; median 90-day health-system cost $2,279 (IQR $512–$4,828, inflation-adjusted 2017 dollars); benign median $2,203; cancer median $21,039. pubmed.ncbi.nlm.nih.gov/40067756/
33. FDA. Labeling changes for six menopausal hormone therapy products. February 12, 2026 — removed cardiovascular, breast cancer, and dementia boxed warnings; endometrial cancer warning for systemic estrogen-alone retained. fda.gov
34. ACOG Clinical Consensus. Compounded Bioidentical Menopausal Hormone Therapy. 2023 — data inadequate to assess endometrial cancer risk.
35. NASEM. The Clinical Utility of Compounded Bioidentical Hormone Therapy. 2020 — low-dose progesterone has not been found to protect the endometrium.
37. British Menopause Society. Compounded transdermal progesterone review. May 2026 — variable absorption; may not provide sufficient endometrial protection (transdermal route specifically).
39. The Menopause Society. Position statement on compounded bioidentical hormone therapy — not recommended for menopause symptoms.
This page contains affiliate links. See our full affiliate disclosure. · Corrections policy. · Consumer health data privacy.
Last verified: July 2026. The HRT Index editorial team. Not a substitute for professional medical advice.