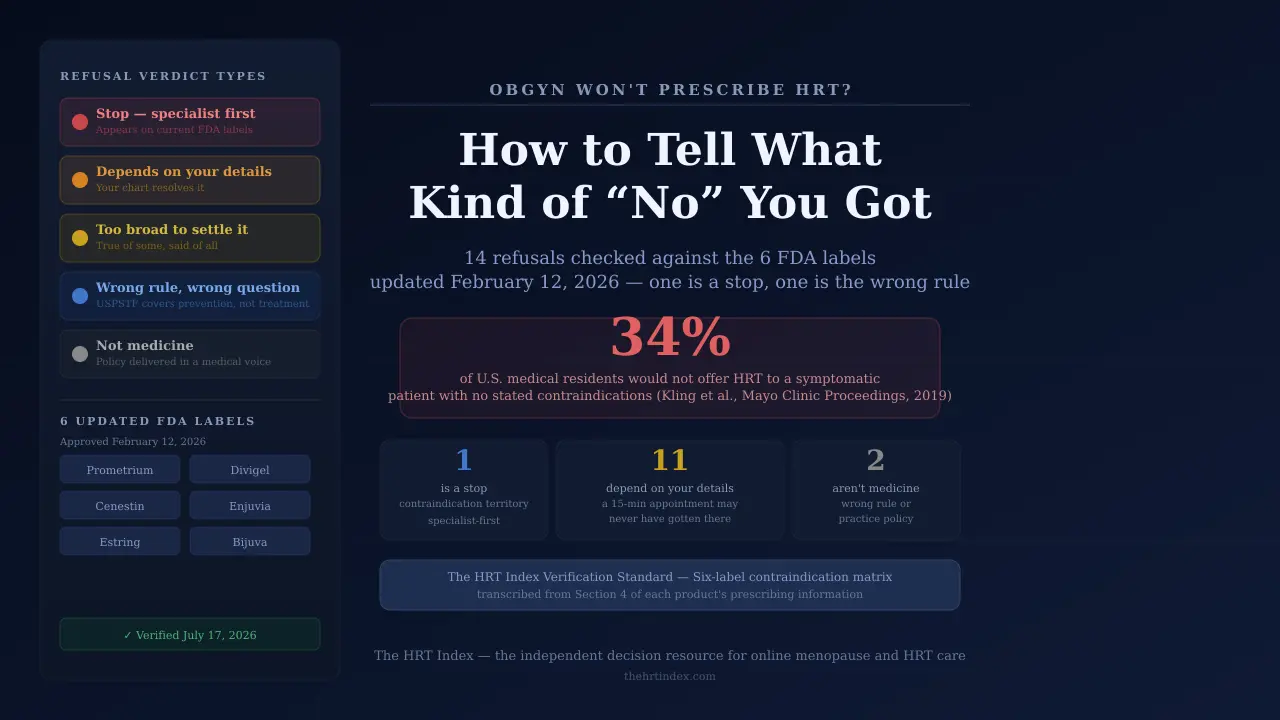
We took the fourteen refusals women report most often and checked each one against the six FDA prescribing labels updated on February 12, 2026. One of the fourteen groups together the issues that need a specialist first. One is a guideline about a completely different question — and if that’s the one you got, the guideline itself says, in writing, that it doesn’t cover you. One isn’t a medical reason at all. The other eleven depend on facts about you that a fifteen-minute appointment may never have gotten to.
In a survey of 183 U.S. medical residents, respondents were given a vignette: a symptomatic, newly menopausal woman with no stated contraindications. 63 of them — 34.4% — said they would not offer her hormone therapy (Kling et al., Mayo Clinic Proceedings, 2019). The study didn’t ask why. It just recorded the answer.
One in three. On a woman with nothing in the way.
This page is for you if:
- ✓You were told no recently and the reason didn’t make sense.
- ✓You want to know whether to push back, get a second opinion, or let it go.
- ✓You’re willing to hear that sometimes the answer really is no.
This page is not for you if:
- ✗You want to be told your doctor is an idiot. We don’t know your chart. She might be completely right.
- ✗You’re looking for a way to leave something out of your history to get a prescription. Don’t. We’ll explain why.
- ✗You haven’t decided whether you want HRT yet — start with what HRT actually is and does.
The HRT Index is the independent decision resource for online menopause and HRT care — comparing telehealth providers on clinical legitimacy, care quality, medication fit, price transparency, and access, with every claim verified and dated, so women can choose the path that fits their situation before their first consult.
What do the 14 common HRT refusals actually mean?
Fourteen sentences account for most reported HRT refusals. One groups together the safety issues that call for specialist-led evaluation before systemic hormone therapy. One is a preventive-care guideline that does not address symptom treatment. One is a practice policy rather than a clinical finding. The remaining eleven depend on patient-specific details that a short appointment may not have covered.
Every other page on this topic lists reasons doctors have. This one lists sentences you heard, and checks each against a source you can open yourself.
How to read the verdict column:
- StopAppears on one or more current FDA labels or needs clinician-led evaluation. Don’t shop for a prescriber. Get the issue evaluated.
- DependsIt can genuinely matter. The sentence alone doesn’t settle it.
- Too broadTrue of some women, said as if it’s true of all women.
- Wrong ruleA real guideline, applied outside what it covers.
- Not medicineA policy or a preference, delivered in a medical voice.
The Refusal Decoder
| What she said | Verdict | What it usually means | Your next sentence |
|---|---|---|---|
| “You’re too young — you’re still having periods” | Depends | Perimenopause is usually assessed from age, menstrual history, and symptoms rather than from waiting for periods to stop (NIH). But pregnancy is still possible while you’re cycling, and contraception, bleeding patterns, and other diagnoses genuinely matter. Continuing periods aren’t listed as a contraindication in any of the six February 2026 labels — though label silence isn’t the same as eligibility. | “Is my age the reason, or are you concerned about contraception, bleeding, or another diagnosis?” |
| “Your hormone levels came back normal” | Too broad | FSH and estradiol both swing during perimenopause — a single result is a snapshot, and one draw shouldn’t be used alone to rule the transition in or out (NIH). | “Are you ruling out perimenopause on one result? What else would explain my symptoms?” |
| “HRT causes breast cancer” | Too broad | The class-wide sentence is too broad to act on. On February 12, 2026, the FDA approved label changes removing the breast cancer, cardiovascular disease, and probable dementia risk statements from the boxed warning of six products (FDA). Breast cancer risk information still appears elsewhere in current prescribing information, and it’s read against product, regimen, duration, and your history. | “Which specific risk, which product, and which part of my history?” |
| “You’re over 60 / more than 10 years out” | Depends | A real risk-stratification factor — and a benefit-risk framework, not an eligibility rule. Current FDA and menopause guidance describe a more favorable balance for appropriate symptomatic women starting systemic therapy before 60 or within ten years of menopause onset (FDA). The Menopause Society says therapy shouldn’t be routinely stopped solely because a woman reaches 60 or 65 (The Menopause Society). | “Are we talking about starting now or continuing? And what about local vaginal estrogen?” |
| “Your family history of breast cancer rules it out” | Depends | The systemic labels contraindicate current or pastbreast cancer — personal, not family. Family history is part of your risk picture, not an automatic disqualifier. Genetic findings like BRCA change the conversation. | “Which line on the label applies to me specifically?” |
| “Your clot risk / your BMI / your migraines” | Depends + route | A risk factorisn’t the same as having had the event. And your doctor may be objecting to oral estrogen specifically without saying so. See the route section. | “Was that about estrogen generally, or oral estrogen specifically? Would transdermal change your assessment?” |
| “You have a uterus, so you can’t take estrogen” | Too broad | Having a uterus usually changes the regimenwhen systemic estrogen is used, because endometrial protection generally has to be addressed. That’s not the same as ruling out every option. The FDA is keeping the endometrial cancer boxed warning on systemic estrogen-alone products (FDA). | “Is the concern unopposed estrogen? What protection options fit me?” |
| “Once you start, you can’t stop” | Too broad | There’s no rule requiring lifelong use. Hormone therapy gets re-evaluated periodically. Symptoms can come back after stopping, and any change should be clinician-guided — but “you can never stop” isn’t a thing. | “What would our re-evaluation plan look like?” |
| “HRT is only for hot flashes” | Too broad | Established uses also include genitourinary syndrome of menopause (GSM — vaginal and urinary symptoms from low estrogen), primary ovarian insufficiency, and bone-loss prevention in appropriate women. It is not for anti-aging, weight loss, or preventing heart disease or dementia. | “Which of my symptoms are you evaluating? Are systemic and local being considered separately?” |
| “Your symptoms aren’t severe enough” | Depends | Not everyone needs HRT. But “severe enough” isn’t a defined threshold — it’s a judgment. It should account for how your life is actually going. | “How are we measuring the effect on my daily life? What threshold are you using?” |
| “Try birth control or an antidepressant first” | Depends | This can be a genuinely good call. Contraception may still be necessary in perimenopause, and hormonal contraceptives affect cycles and symptoms too. Certain antidepressants are established non-hormonal options for hot flashes. What ’s missing when it’s a brush-off is the why. | “What goal does this treat — contraception, bleeding, hot flashes, mood? How do the tradeoffs compare?” |
| “The USPSTF recommends against hormone therapy” | Wrong rule | The U.S. Preventive Services Task Force recommendation addresses systemic hormone therapy for the primary prevention of chronic conditions in asymptomatic postmenopausal people. It does not address hormone therapy used to treat menopausal symptoms (USPSTF). If you came in with symptoms, you came in with a question the recommendation doesn’t answer. | “Are you applying the prevention recommendation, or evaluating treatment for my symptoms?” |
| “I don’t prescribe HRT” / “we don’t do that here” | Not medicine | Scope, comfort, training, or practice policy — said as if it were a finding about you. It may be a completely honest answer. It just isn’t a medical reason. | “Is that a policy of the practice, or a conclusion about my history? Will you refer me?” |
| “You have a history of breast cancer / a blood clot / a stroke / liver disease / unexplained bleeding” | Stop — specialist first | These appear across the six labels updated in February 2026 — though not identically on all six, which matters more than you’d think. The product-level table is here. | Read that section. Then talk to your oncologist or specialist — not a telehealth intake form. |
In the competing pages and sources we reviewed on July 17, 2026, we didn’t find this sentence-by-sentence structure anywhere else. That’s why we built it.
The right online HRT provider isn’t the same for every woman — it depends on your symptoms, your age and whether you have a uterus, your medication route preference, your risk history, your insurance, and your state.
Use The HRT Index’s Find My HRT Path tool to match your situation to the right provider — and to flag when online care isn’t the right starting point — before your first consult.
Get your personalized action plan →Free. No email needed to see your result.
Why did your OBGYN say no?
Two U.S. residency surveys have documented substantial gaps in menopause education. Among 177 residents responding to one survey, 12 (6.8%) felt adequately prepared to manage menopause and 36 (20.3%) reported no menopause lectures at all. A separate survey of 99 responding OB-GYN residency program directors found 31.3% reported a menopause curriculum. These are population-level findings and cannot explain any individual clinician’s decision.
That last sentence matters, so we’ll say it plainly before anything else: these numbers describe a system. They can’t tell you what happened in your appointment. Your doctor may have had a specific, correct reason she didn’t explain well. Anyone who tells you otherwise from a webpage is guessing.
In 2002, the Women’s Health Initiative published findings on specific oral regimens in a study population averaging about 63 years old — more than a decade past the average age of menopause. The Menopause Society reports use among U.S. postmenopausal women falling from 26.9% in 1999 to 4.7% in 2020 (The Menopause Society).
The FDA has described the original warning as resting on a statistically non-significant increase in breast cancer diagnosis, in a study population well past the average age of menopause, given a hormone formulation the agency says is no longer in common use (FDA, November 10, 2025). Among the OB-GYN residency programs that reported having a menopause curriculum, 71% reported two or fewer menopause lectures per year (The Menopause Society).
She got fifteen minutes with you. She’s working from what she was taught, what she’s read since, and possibly from a printed label that hasn’t been updated yet. She may not be the villain of this story. Walking back in angry gets you nowhere. Walking back in with a specific questiongets you a different conversation entirely. That’s not us being nice. That’s us telling you what works.
What changed in FDA HRT boxed warnings in 2026?
On November 10, 2025, the FDA initiated removal of boxed-warning risk statements on cardiovascular disease, breast cancer, and probable dementia from menopausal hormone therapy products. On February 12, 2026, it approved the first six updated labels: Prometrium, Divigel, Cenestin, Enjuvia, Estring, and Bijuva. Twenty-nine drug companies submitted proposed changes at the FDA’s request. The action changed boxed-warning language on those six products. It did not remove every boxed warning, every risk statement, or every product’s existing label.
What everyone says: the FDA removed the black box warning from HRT.
What’s actually true: the FDA removed three risk statements from the boxed warnings of six products (FDA, February 12, 2026). We checked the FDA’s tracking page on July 17, 2026. It was still stamped “Content current as of: 02/12/2026,” and it still listed exactly six products (FDA). Six. Twenty-nine companies filed.
What the FDA’s page listed when we checked it
| Product | Category | Boxed warning statements removed? | Label |
|---|---|---|---|
| Prometrium (progesterone capsules) | Progestogen alone | Yes — Feb 2026 | Label PDF |
| Divigel (estradiol gel) | Systemic estrogen alone | Yes — Feb 2026 | Label PDF |
| Cenestin (synthetic conjugated estrogens, A) | Systemic estrogen alone | Yes — Feb 2026 | Label PDF |
| Enjuvia (synthetic conjugated estrogens, B) | Systemic estrogen alone | Yes — Feb 2026 | Label PDF |
| Estring (estradiol vaginal system) | Topical vaginal estrogen | Yes — Feb 2026 | Label PDF |
| Bijuva (estradiol + progesterone capsules) | Systemic estrogen + progestogen | Yes — Feb 2026 | Label PDF |
| Generic estradiol, Estrace, Climara, Vivelle-Dot, Premarin, Prempro, EstroGel, Vagifem, Imvexxy, and others | All categories | Not listed on the FDA’s updated-prescribing-information page as of July 17, 2026 | |
The FDA described these six as the first batch. Its public materials don’t publish a product-by-product timeline for the remaining submissions. We re-check this page monthly — check it yourself before you rely on the table.
Why this matters more than anything else here
The product your doctor would actually write for may not have an updated label yet. Most of the ones she reaches for weren’t on the FDA’s list when we checked.
That’s not laziness. That’s a queue.
What did not change
- ⚠Removing a statement from a boxed warning is not the same as removing the risk information. Breast cancer, cardiovascular, thrombotic, and other risk information still appears elsewhere in current prescribing information. The February action changed where and how three statements appear on six labels. It did not declare hormone therapy risk-free.
- ⚠The endometrial cancer warning stays.The FDA did not seek removal of the endometrial-cancer boxed warning from systemic estrogen-alone products. If you have a uterus, that’s unchanged.
- ⚠The Menopause Society was more careful than the press release. It agreed with removing the boxed warning on low-dose vaginal estrogen. But on systemic estrogen it said risks remain in certain individuals; that risks are low for younger, healthy women starting closer to the transition; and that risks are greater in older women and those further from menopause onset (The Menopause Society, November 14, 2025).
- ⚠ACOG’s president pushed back on lumping the products together. He commended removing the warning for low-dose vaginal estrogen, but said systemic estrogen medications have a different safety profile and that long-term use may still carry a slightly elevated risk of breast cancer.
When is an OBGYN right to refuse HRT?
Certain conditions appear as contraindications on the FDA labels updated February 12, 2026 — but not identically across products. Unexplained vaginal bleeding, active or prior blood clots, active or prior stroke or heart attack, and liver disease appear on all six. Breast cancer history, estrogen-dependent tumors, and inherited clotting disorders appear on some and not others. If one of these describes you, the next step is clinician-led evaluation, not a search for a different answer.
There is no single “FDA label” for HRT. There are six updated ones, and their contraindication lists are different. That difference is not a technicality. It’s the whole reason the systemic-versus-local question exists.
Which contraindication appears on which label
| Contraindication (plain English) | Divigel (gel) | Cenestin (pill) | Enjuvia (pill) | Bijuva (capsule) | Prometrium (prog.) | Estring (vaginal) |
|---|---|---|---|---|---|---|
| Vaginal bleeding no one has explained yet | Yes | Yes | Yes | Yes | Yes | Yes |
| Breast cancer now or in your past | Yes | Yes | Yes | Yes | Yes (known, suspected, or history) | Not listed |
| A tumor that grows on estrogen | Yes | Yes | Yes | Yes | Not listed | Yes (known or suspected) |
| A blood clot in your leg or lung — now or in your past | Yes | Yes | Yes | Yes | Yes | Yes |
| A stroke or heart attack — now or in your past | Yes | Yes | Yes | Yes | Yes | Yes |
| Liver disease or impaired liver function | Yes | Yes | Yes | Yes | Yes | Yes |
| An inherited clotting disorder (protein C, protein S, or antithrombin deficiency) | Yes | Yes | Yes | Yes | Not listed | Yes |
| A severe allergic reaction to the product | Yes | Yes | Yes | Yes | Yes | Yes |
| A peanut allergy | — | — | — | — | Yes — contains peanut oil | — |
Transcribed from Section 4 of each product’s current prescribing information, verified July 17, 2026. Label links are in the FDA table above. Labels change — check the PDF before you rely on this.
Read the Prometrium column.If you have a peanut allergy and your doctor said no to Prometrium specifically, that’s why. It has nothing to do with hormones.
Now read the Estring row.Estring’s contraindication list doesn’t include breast cancer history the way the four systemic products do. That is a fact about a label. It is not permission. What that row actually tells you is: systemic and local are different questions with different answers, and a refusal that lumps them together hasn’t answered either one.
If you have a history of breast cancer
A personal history of hormone-receptor-positive breast cancer is a specialist-first situation. Systemic estrogen is generally considered contraindicated in that setting, and it appears on the systemic labels above. Any decision about treating your symptoms should be coordinated with your oncology team. Please don’t go looking for a telehealth clinic that will say yes.
But the local question is a real one with real guidance behind it. ACOG’s clinical consensus on urogenital symptoms after estrogen-dependent breast cancer supports non-hormonal approaches first. If those haven’t given adequate relief, low-dose vaginal estrogen can be considered through shared decision-making with your care team (ACOG Clinical Consensus, 2021).
The move here is a conversation with your oncologist about your vaginal and urinary symptoms. Not an intake form. Not this page. Your oncologist. Ask specifically: “Have we exhausted the non-hormonal options, and if so, is local therapy something we can discuss?”
Please don’t do these two things
Don’torder a hormone product from Amazon or unapproved channels. Unapproved or unverified hormone products sold outside legitimate prescription channels aren’t evaluated the way FDA-approved prescription drugs are, and nobody is checking them against your history.
Don’t leave things out of your history to get a yes.If you skip the clot, or the bleeding, or the cancer, the clinician on the other end can’t do the one job you actually need them to do. A second opinion is a fresh evaluation. It isn’t a way to beat the first one.
No call to action in this section. If this is you, we don’t want your click. We want you to call your oncologist.
Is vaginal estrogen different from systemic HRT?
Systemic hormone therapy and local vaginal estrogen are different treatment categories with different exposure levels, different indications, and — as the six updated FDA labels show — different contraindication lists. Estring’s contraindications do not include breast cancer history the way the systemic products’ do. A decision about systemic therapy does not automatically settle the question of local therapy.
Systemic therapy— pills, patches, gels, sprays — is meant to work throughout your body. It’s what treats hot flashes and night sweats, and what’s used for bone-loss prevention in appropriate women.
Local vaginal estrogen— rings, creams, tablets, inserts — is aimed at vaginal and urinary symptoms. Doctors call that cluster genitourinary syndrome of menopause (GSM): dryness, burning, pain with sex, urgency, recurrent UTIs.
Local products still have some systemic absorption, and Estring’s label says the relevance of systemic risks at that lower exposure isn’t settled. But they aren’t the same question either. The FDA’s own action treats them as separate categories, and both The Menopause Society and ACOG’s president specifically distinguished low-dose vaginal estrogen from systemic estrogen when they responded to the February change.
If your main problem is dryness, pain with sex, or recurrent UTIs — and you got a blanket “no HRT” — you may have received an answer to a question you didn’t ask. Go back with:
“I want to talk specifically about local vaginal estrogen for my vaginal and urinary symptoms. Is your concern about systemic therapy, or does it apply to local treatment too?”Do you need blood tests before HRT?
Perimenopause and menopause are usually assessed from age, menstrual history, and symptoms rather than from hormone testing, because FSH and estradiol fluctuate and a single result is difficult to interpret. Testing may still be appropriate when symptoms begin unusually early, when menstrual history is unclear, or when another condition needs to be investigated.
If your refusal was “your levels came back normal,” this section is your whole argument.
Why one test may not answer it.During perimenopause, FSH and estradiol don’t decline in a tidy line. They rise and fall — sometimes within a single cycle. A draw on Tuesday can read one way and a draw the following week can read another (NIH).
Why your doctor might still want labs. Testing gets useful when it would actually change what happens next:
- Symptoms started unusually early
- Your menstrual history is unclear (hysterectomy, ablation, certain IUDs)
- She’s ruling out something that looks like perimenopause but isn’t — thyroid disease, anemia, medication effects, pregnancy
- There’s bleeding that needs explaining
Use the perimenopause symptom checklist before your next appointment →
Does the patch instead of the pill change your risk?
A 2010 meta-analysis of observational studies reported pooled venous thromboembolism risk ratios of 1.9 (95% CI 1.3–2.3) for oral estrogen users and 1.0 (95% CI 0.9–1.1) for transdermal users. Oral estrogens increase thrombin generation and induce resistance to activated protein C; transdermal estrogens have minimal effect on those measures. These are observational findings and do not establish that any route is appropriate for a specific individual.
Read those two numbers again. 1.9 for the pill. 1.0 for the patch— and the transdermal confidence interval crosses no increase at all (Canonico & Scarabin, Curr Opin Hematol, 2010). Estrogen you swallow goes through your liver first, and the liver responds by making more clotting proteins. Estrogen through your skin — patch, gel, spray — skips that first pass.
Which means a refusal built on clot risk may have answered a question you never asked. You asked about hormones. The answer may have been about pills.
What kind of clot concern did she mean?
| What’s in your history | Listed contraindication? | Route part of conversation? | Where to start |
|---|---|---|---|
| A prior DVT or PE (clot in leg or lung) | Yes — on all six labels | No. This is a stop, not a route question. | Specialist. |
| A prior stroke or heart attack | Yes — on all six labels | No. | Specialist. |
| A known inherited clotting disorder (protein C, protein S, antithrombin deficiency) | Yes — on five of six (not listed on Prometrium) | No. | Specialist. |
| Family history of clots only — no personal event | Not listed as a contraindication | Possibly — part of a fuller risk assessment | Ask which fact she’s weighing |
| BMI, smoking, or another risk factor — no clot event | Not listed as a contraindication | Possibly | Ask about route |
| Migraine without aura | Not listed as a contraindication | Possibly | Ask about route and dose |
| Migraine with aura | Not listed, but relevant to vascular risk | Likely part of it — aura, dose, route, and other vascular risk factors get weighed together | Ask for the individualized assessment |
What this table can’t do: tell you which column you’re in. Only someone with your chart can.
“Was your concern about estrogen generally, or about oral estrogen specifically? Would transdermal change your assessment?”
What should you say at your next appointment?
Asking for a specific reason produces more useful information than asking for a specific prescription. The goal of a follow-up conversation is to leave with a documented reason, clarity on whether it covers systemic or local therapy, and a plan for evaluation, alternatives, or referral.
Before you pay anyone for a second opinion, try the doctor you already have. She has your chart. She has your labs. She has your history. And a specific question often gets a different answer than a general request.
The four questions
- 1
“Is there a specific contraindication in my chart, or is this a general concern?”
This is the whole page in one sentence. It forces the distinction between a fact about you and a feeling about hormones.
- 2
“Does that concern apply to systemic HRT, local vaginal estrogen, or both?”
Different categories. Different labels. Most refusals never separate them.
- 3
“Was that about estrogen generally, or oral estrogen specifically?”
The route question — but only if you’re in the right rows of that table.
- 4
“If not HRT, what’s the plan for these symptoms?”
This one makes “no” cost something. A no with no plan attached isn’t a treatment decision — it’s the end of the appointment.
Ask her to write it down
Not as a threat. Not as a malpractice hint. You just need the reason in writing to take anywhere else.
Bring specifics, not adjectives
- Night sweats per week
- How many times you wake up
- Work you’ve missed, or meetings you’ve lost the thread in
- Pain during sex
- Your bleeding pattern
- What you’ve already tried, and what happened
“I’m exhausted” is easy to file under stress. “I’m waking up four times a night, soaked, and I’ve missed two deadlines this month” is a clinical picture.
What a real answer sounds like vs. a brush-off
| Real answer | Brush-off |
|---|---|
| “Your DVT in 2019 — that’s on the label as a contraindication.” | “It’s just not something I’d recommend.” |
| “Let’s rule out thyroid first, then revisit in six weeks.” | “Let’s wait and see.” |
| “I don’t manage this. Dr. Chen down the hall does. I’ll send the referral.” | “You’re too young for this.” |
Not sure which of the fourteen you got?
You’ve got the questions. Now match them to your actual situation — your symptoms, your age and whether you have a uterus, your risk history, your insurance, and your state. The HRT Index’s Find My HRT Path tool does that in about ninety seconds, and it will tell you straight when online care isn’t the right starting point.
Get your personalized action plan →Free. No email needed to see your result.
What if your OBGYN still won’t prescribe HRT?
Three second-opinion routes exist: an in-person clinician credentialed in menopause medicine, telehealth that bills commercial insurance, or cash-pay telehealth. The right route depends on the reason for the refusal, whether you have insurance, and whether the specific product you need is available through that route. A second opinion is a new clinical evaluation and may also result in a refusal.
That last sentence is the honest one. Nobody can promise you a yes. Anyone who does is selling. But if your reason came back “too broad,” “depends on your details,” “wrong rule,” or “not medicine” — a second opinion is a completely reasonable thing to want.
Which route fits which refusal
| Your situation | Start here | Why |
|---|---|---|
| Reason was clear, follow-up plan exists | Your current doctor | Don’t pay for a second opinion you don’t need |
| “I don’t prescribe HRT” / no referral offered | MSCP directory, or insurance-billing telehealth | Access problem, not a medical one |
| “Too young” / “levels are normal” / “USPSTF” | Any menopause-trained clinician | You need someone who reads the current guidance |
| Clot risk factors, BMI, migraines — no clot event | Menopause-trained clinician; ask about route | You need the transdermal conversation |
| Mainly vaginal or urinary symptoms | Menopause-trained clinician; ask about local therapy | Different question, different answer |
| Unexplained bleeding | Clinician-directed evaluation, often in person | Needs explaining before an online prescribing route |
| Breast or endometrial cancer history | Oncologist first | Coordination, not telehealth |
| Prior clot, stroke, heart attack, liver disease | In-person or relevant specialist | Contraindication territory |
| No insurance, cash-pay, want price certainty | Cash-pay telehealth | Compare below |
Path 1: A Menopause Society Certified Practitioner — try this first
Free to search — we earn nothing from it
The Menopause Society Certified Practitioner (MSCP) credential goes to licensed clinicians who pass a competency exam in menopause and midlife women’s health. It’s valid for three years and maintained by re-examination or continuing education.
The Society runs a Find a Menopause Practitioner directory. Two honest caveats, straight from the Society itself: it isn’t a complete list — it includes only members and MSCPs who asked to be included and are accepting new patients — and the Society doesn’t endorse or recommend the clinicians in it.
The real downside: waitlists, and thin coverage outside metro areas. If you’re rural, this may not be a real option this month. We’re telling you to try the free thing first because for a lot of you it’s the right answer. If it works, close this tab. Genuinely.
Path 2: Telehealth that bills your insurance — Midi Health
Paid partnership — we may earn a commission
This is the route that matches what you originally walked in asking for: a normal prescription, for an FDA-approved medicine, filled at your pharmacy, run through your insurance.
Midi does not bill Medicaid.Midi says it and its medical groups are not enrolled with state healthcare programs and cannot treat Medicaid or Medi-Cal patients — not even as self-pay. Midi says it is not covered by Medicare; beneficiaries can be seen as self-pay but cannot submit those visits to Medicare (Midi, checked July 17, 2026).
If that’s you, Midi is out. Search for HRT on Medicaid or HRT on Medicare options instead.
| Item | Midi states | We independently checked |
|---|---|---|
| Insurance | In-network with most major insurance providers; most PPO plans. Coverage varies by plan. | Read on Midi’s public pricing and insurance page, July 17, 2026. We did not verify any individual plan’s network status. |
| Self-pay | $250 initial visit / $150 continued care visits | Provider-published, July 17, 2026 |
| Medication | Prescribes FDA-approved hormonal treatments through standard pharmacies | Provider-stated. A telehealth service is not itself FDA-approved. Confirm the exact product prescribed. |
| Clinicians | Menopause-trained, including MSCPs | Provider-stated; named clinicians listed publicly |
| Hard exclusion | No Medicaid/Medi-Cal at all. Not covered by Medicare. | Read directly from Midi’s pricing page, July 17, 2026 |
Patient story (published by Midi, not independently verified): Katherine G. said “Midi was incredibly easy. I signed up and had a visit the next day.” This says nothing about typical access, results, or whether you’d be eligible for medication.
Our editorial read:if your refusal landed in “too broad,” “wrong rule,” or “not medicine,” and you have commercial coverage, Midi is the route on this page that most directly reproduces what you asked your OBGYN for. That’s a judgment based on the facts in the table above — insurance model, medication category, and clinician credentialing.
Does that sound like your situation?
Check Midi’s current state availability and whether your plan is listed in network →Takes about a minute and costs nothing. If your plan isn’t listed, you’ll know before you book.
Paid link — we may earn a commission. It doesn’t change what you pay, or what we concluded.
Path 3: Cash-pay telehealth — Winona
Paid partnership — we may earn a commission
For the woman with no insurance who wants to see the price before she talks to anyone. Winona advertises a free initial online evaluation, and every product is priced on the site before you enter a card.
Winona carries a mixed formulary.Its public pages identify some product categories — certain patches, tablets, and progesterone capsules — as FDA-approved, and identify its compounded creams as not FDA-approved. Winona’s pharmacy page states its products are prepared by 503A compounding pharmacies. The finished compounded drugs are not FDA-approved.
ACOG’s position is that compounded bioidentical menopausal hormone therapy should not be prescribed routinely when FDA-approved formulations exist (ACOG Clinical Consensus No. 6, 2023). Compounded is not the same as FDA-approved. It is not “more natural.” Anyone telling you otherwise is marketing at you.
If you use Winona, ask exactly this: “Which commercial product, from which manufacturer, would actually be dispensed to me?”
Winona’s published prices (checked July 17, 2026):
| Product | Published “from” price | Status |
|---|---|---|
| Progesterone Capsules | From $39/month | Provider-stated FDA-approved category; confirm manufacturer before purchase |
| Estrogen Tablets | From $54/month | Provider-stated FDA-approved category; confirm manufacturer before purchase |
| Estrogen Body Cream (with Progesterone) | From $89/month | Compounded — not FDA-approved |
| Vaginal Estrogen Cream | From $89/month | Compounded — not FDA-approved |
| Estrogen Patch | From $149/month | Provider-stated FDA-approved category; confirm manufacturer before purchase |
| Initial online evaluation | Advertised free | Medication subscription charges apply if treatment is prescribed |
Every price above is a published “from” price read off Winona’s product page on July 17, 2026. We did not complete a checkout. Confirm your actual recurring total before you buy.
If that fits what you’re looking for:
See Winona’s current published prices and medication categories →The evaluation is free and the prices are on the page. Ask which manufacturer’s product would be dispensed.
Paid link — we may earn a commission. It doesn’t change what you pay, or what we concluded.
Path 4: Cash-pay visits, prescription to your own pharmacy — Sesame Care
Worth knowing if you’re uninsured for visits but insured for pharmacy
Sesame is a clinician marketplace with a menopause-care subscription. You choose a named clinician, pay cash for a video visit, and if a prescription is appropriate it goes to the pharmacy you choose — where your own insurance formulary applies. Sesame states it doesn’t bill insurance for the visit, medication costs are separate, and basic labs may be included when clinically ordered. Its direct page advertised from $59/month when we checked (Sesame, July 17, 2026).
Two honest limits. Sesame’s Costco-indexed materials showed conflicting monthly figures when we checked, so don’t treat any discount price as settled until you see it in the live checkout. And because Sesame is a marketplace, the clinician you pick determines how much menopause experience you get. Check the clinician’s profile before you book.
Read our full Sesame Care review for a deeper comparison.Also in the market: Hers
Hers lists estradiol pill or patch and progesterone for menopause and perimenopause. Two things to know before you start: Hers states the service is not available in all 50 states, and states that treatment of perimenopausal symptoms may be off-label— meaning the medicine is FDA-approved, but not specifically approved for that use (Hers, checked July 17, 2026). Off-label prescribing is legal, common, and normal in medicine. You should still know when it’s happening to you.
Compare all online menopause providers in our full provider roundup.
What none of these can do for you
- ✗None can treat a real contraindication. The label doesn’t care which website you used.
- ✗None can examine you. Unexplained bleeding needs a clinician who can evaluate it.
- ✗None replaces an oncologist.
- ✗Midi can’t take Medicaid.
- ✗All of them can say no too. A service that can’t say no is a service you shouldn’t want.
What if systemic HRT isn’t right for you?
A decision against systemic hormone therapy does not end the treatment conversation. Depending on the symptom, history, and diagnosis, the next discussion may involve local vaginal therapy, an evidence-based non-hormonal prescription medicine, treatment of another condition, or symptom-specific supportive care.
“Not appropriate” is not the same as “nothing can be done.” That’s the sentence that gets lost, and it’s the one that leaves women suffering for years.
1. Local therapy may still be a separate conversation.
If your worst symptoms are vaginal or urinary, the local question hasn’t necessarily been answered by a systemic refusal. See the section above.
2. There are established non-hormonal prescription options for hot flashes.
The NIH identifies certain antidepressants, gabapentin, oxybutynin, and neurokinin-3 receptor antagonists among options used for vasomotor symptoms (NIH). We’re naming the categories, not telling you which to ask for — that’s a conversation with a clinician who knows your history.
3. It might not be menopause.
Thyroid disease, anemia, sleep disorders, and medication effects all overlap with the symptom picture. If nobody has looked, that’s worth asking about — and it’s the one scenario where your doctor’s caution may have been protecting you from a wrong diagnosis, not from a drug.
- Non-hormonal menopause treatments (covered in our non-hormonal treatment guide)
- Veozah and the non-hormonal drug class (fezolinetant, the NK3 receptor antagonist)
- Vaginal estrogen and local therapy →
Why is your estradiol patch backordered?
As of our July 2026 check, the American Society of Health-System Pharmacists listed an estradiol transdermal system shortage while estradiol patches were not on the FDA’s national drug shortage list. The two organizations use different definitions, reporting channels, and thresholds, so an ASHP listing can coexist with the absence of an FDA-declared national shortage.
We just spent a whole section telling some of you to ask about the patch. Here’s what happens next for a lot of you: you win the argument, you walk into the pharmacy, and they tell you it’s on backorder. Both official answers are true.
| FDA | ASHP | |
|---|---|---|
| What it says | Estradiol patches are not on the national drug shortage list; manufacturers report producing at capacity | Lists an estradiol transdermal system shortage (ASHP) |
| Where the data comes from | Manufacturers | Practitioners, pharmacists, physicians, nurses, patients and caregivers |
| So it’s measuring | How much is being made | How many people reported they couldn’t get it |
What to do about it
- ›Call around before you panic. A different manufacturer or a different patch schedule may be sitting on a shelf two miles away. Availability varies by pharmacy.
- ›Ask your prescriber about gel or spray.Both are transdermal — they skip the liver the same way a patch does. Divigel is one of the six products with an updated FDA label.
- ›Don’t cut a patch unless you’ve confirmed you can. Patch designs differ, and cutting the wrong kind changes the dose you actually absorb in unpredictable ways. Ask your pharmacist or prescriber about your specific product before you cut anything.
- ›Oral is still an option— but if a patch was chosen specifically because of clot risk factors, that ’s exactly the conversation to have first. See the route section.
Will insurance cover HRT from a second-opinion clinician?
Coverage depends on your health plan, the clinician’s network status, the exact product and NDC prescribed, the indication, the formulary tier, prior authorization requirements, quantity limits, and the dispensing pharmacy. FDA approval does not guarantee coverage. Compounded-drug reimbursement is plan-specific and is often limited.
Short version: the medicine matters, but the plan decides.
What generally moves in your favor:an FDA-approved product, prescribed by a clinician your plan recognizes, filled at an in-network pharmacy, for a covered indication. That’s the same footing you’d have been on if your OBGYN had written it. What generally doesn’t:compounded hormones. Confirm your plan’s exclusion and reimbursement rules before you pay, not after.
What if your insurance denies it or wants prior authorization?
A denial isn’t always the end. It’s frequently a paperwork problem wearing a scary hat. Ask your plan these, in this order:
- “What’s the exact reason for the denial?” Get the code. Not the vibe.
- “Is the specific product on formulary, and at what tier?” A different strength or manufacturer’s version of the same drug is sometimes covered when yours isn’t.
- “Is prior authorization required, and what does it need?” Usually your clinician’s office submits it. Ask them to.
- “Is there a step-therapy requirement?” Some plans want you to try a preferred option first.
- “Is there a quantity limit?”This catches people whose prescription is fine but whose day-supply isn’t.
- “Is the pharmacy in network?” Same drug, different counter, different answer.
- “What’s the appeal process and the deadline?” There’s almost always one, and it’s almost always shorter than you’d expect.
- HRT insurance coverage: what’s covered and what isn’t →
- Using HSA or FSA funds for HRT (covered in our HRT cost guides)
- What HRT actually costs →
What we actually verified
You should be able to check our work. Here’s exactly what we did — and what we didn’t.
What we independently checked
- ✓ The six updated FDA labels — Section 4 contraindications transcribed product by product, July 17, 2026
- ✓ The FDA’s tracking page for menopausal hormone therapies with updated prescribing information
- ✓ The FDA’s November 10, 2025 announcement and February 12, 2026 approval release
- ✓ The Menopause Society’s position statement materials and November 2025 response
- ✓ ACOG’s clinical consensuses on compounded HRT and urogenital symptoms after breast cancer
- ✓ The USPSTF menopausal hormone therapy recommendation — specifically its stated scope
- ✓ ASHP’s estradiol transdermal system shortage listing and the FDA’s shortage status
What we read but did not independently substantiate
- ⚠ Provider pages. Reading a website verifies what the provider publicly states — not the underlying clinical or formulary claim.
- ⚠ The patient testimonial. Published by Midi. We labeled it as theirs.
What we did not do
- ✗ Review your history
- ✗ Evaluate your doctor
- ✗ Complete any provider intake or checkout
- ✗ Verify any individual insurance benefit, exact dispensed product, NDC, or clinical eligibility
The HRT Index Verification Standard
We evaluate providers on exactly five pillars, always in this order: clinical legitimacy, care quality, medication fit, price transparency, access. We read every published price, separate FDA-approved from compounded, verify state availability and insurance, and re-check on a fixed schedule — top providers monthly, full roster quarterly. We don’t publish numeric provider scores. A number would imply a precision we don’t have.
How we make money:we may earn a commission if you use a paid link on this page. It doesn’t change what you pay, and it didn’t change what we concluded — Path 1 is free and we earn nothing from it, and the section before it tells you to try the doctor you already have.
Read our full affiliate policy → · Report an outdated or incorrect claim →
Frequently asked questions
- Can an OBGYN refuse to prescribe HRT?
- Yes. A clinician isn’t required to prescribe a treatment they believe is inappropriate or outside their practice. Ask for the specific reason, the alternatives, and an appropriate referral, and ask that the reason be documented in your note. A refusal doesn’t prove HRT is unsafe for you — it means this clinician isn’t prescribing it today.
- Does a normal FSH mean I’m not in perimenopause?
- Not necessarily. FSH and estradiol fluctuate during perimenopause, so a single result is difficult to interpret and shouldn’t be used alone to rule the transition in or out. Perimenopause is usually assessed from age, menstrual history, and symptoms. Testing may still be useful when symptoms start unusually early, when your menstrual history is unclear, or when another condition needs investigating.
- Can I take HRT while I’m still having periods?
- Continuing periods aren’t listed as a contraindication in any of the six February 2026 labels. But that absence doesn’t establish that treatment is right for you. Pregnancy is still possible, contraception may still be needed, bleeding patterns matter, and other diagnoses may be in play. Ask whether your cycle status is the actual concern or standing in for one of those.
- Can I start HRT after 60?
- Current FDA and menopause guidance describe a more favorable benefit-risk balance for appropriate symptomatic women starting systemic therapy before 60 or within ten years of menopause onset. That’s a framework, not an eligibility rule, and it doesn’t apply identically to local vaginal therapy. The Menopause Society says therapy shouldn’t be routinely discontinued solely because a woman reaches 60 or 65. Starting later is a more individualized conversation.
- Is a family history of breast cancer a reason to be denied HRT?
- The systemic labels contraindicate current or past breast cancer — personal, not family. Family history is part of your risk picture, not an automatic disqualifier. Bring the details: which relative, what cancer type, their age at diagnosis, and any genetic testing. Those change the conversation.
- Did the FDA remove the black box warning from all HRT?
- No. The FDA removed three risk statements — cardiovascular disease, breast cancer, and probable dementia — from the boxed warnings of six products, approved February 12, 2026. Twenty-nine companies filed proposed changes. Most commonly dispensed products weren’t on the FDA’s updated list when we checked on July 17, 2026. The endometrial cancer boxed warning on systemic estrogen-alone products is staying, and risk information still appears elsewhere in the labels.
- Can I get HRT if I’ve had a blood clot?
- Active or prior blood clots in the leg or lung, and active or prior stroke or heart attack, appear as contraindications on all six labels updated in February 2026. That’s different from having clot risk factors, where route of administration may be part of the assessment. If you’ve had an actual clot, that needs a specialist — not a telehealth intake.
- Can I get HRT online after my local doctor says no?
- A licensed online clinician can evaluate whether treatment is appropriate, where state rules and the service’s model allow it. What that visit should be is a complete second opinion — not a way around a bleeding evaluation, a cancer history, or a clot. If your refusal was “too broad” or “not medicine,” online care is a reasonable route. If it was a listed contraindication, it isn’t.
- Is vaginal estrogen the same as HRT?
- No, and this distinction carries more weight than almost anything else here. Local vaginal estrogen targets vaginal and urinary symptoms at much lower exposure than systemic therapy, and the labels reflect that — Estring’s contraindications differ from the systemic products’. A refusal of systemic therapy doesn’t automatically answer the local question, but most refusals never separate them.
- What if my OBGYN won’t refer me to anyone?
- Ask that the refusal and the reason be documented in your visit note, request your records, and then go around. The Menopause Society’s practitioner directory is free to search. Many telehealth services allow direct booking — though your plan may still require a referral for coverage, which is a separate question from access.
You went in and asked for something reasonable. You got a sentence you couldn’t evaluate. And then you went home and did what women in this position always end up doing — the research, yourself, at 11pm, on your phone.
You shouldn’t have had to. But now you know which of the fourteen you got, what the actual labels say, and what to say next.
That’s the whole fight, honestly.
Still not sure which HRT program is right for you?
Take our free 90-second matching quiz.
Find My HRT Path →The HRT Index is the independent decision resource for online menopause and HRT care — comparing telehealth providers on clinical legitimacy, care quality, medication fit, price transparency, and access, with every claim verified and dated, so women can choose the path that fits their situation before their first consult.
This page is educational and is not medical advice, diagnosis, or treatment. Talk to a qualified clinician about your situation.
Last updated: 2026-07-17 · Last verified: July 17, 2026