Can perimenopause heavy bleeding treatment online actually work?
Answer capsule: Yes, for many women. A virtual clinician can take a history, order a pregnancy test, blood count, and local imaging when appropriate, prescribe treatment, and refer locally. A virtual clinician cannot perform a pelvic exam, take an endometrial sample, insert an IUD, or manage an emergency.
The nine categories — and which ones a screen can find
Doctors worldwide sort abnormal uterine bleeding using a framework called PALM-COEIN, published by FIGO (the International Federation of Gynecology and Obstetrics). Nine cause categories. Two groups. More than one can apply to you at once.
Here's what almost nobody points out: FIGO defines the PALM group as the structural categories you evaluate with imaging and tissue. That's not our opinion about telehealth. That's how the categories were built. Four categories cannot be confirmed from an intake form.
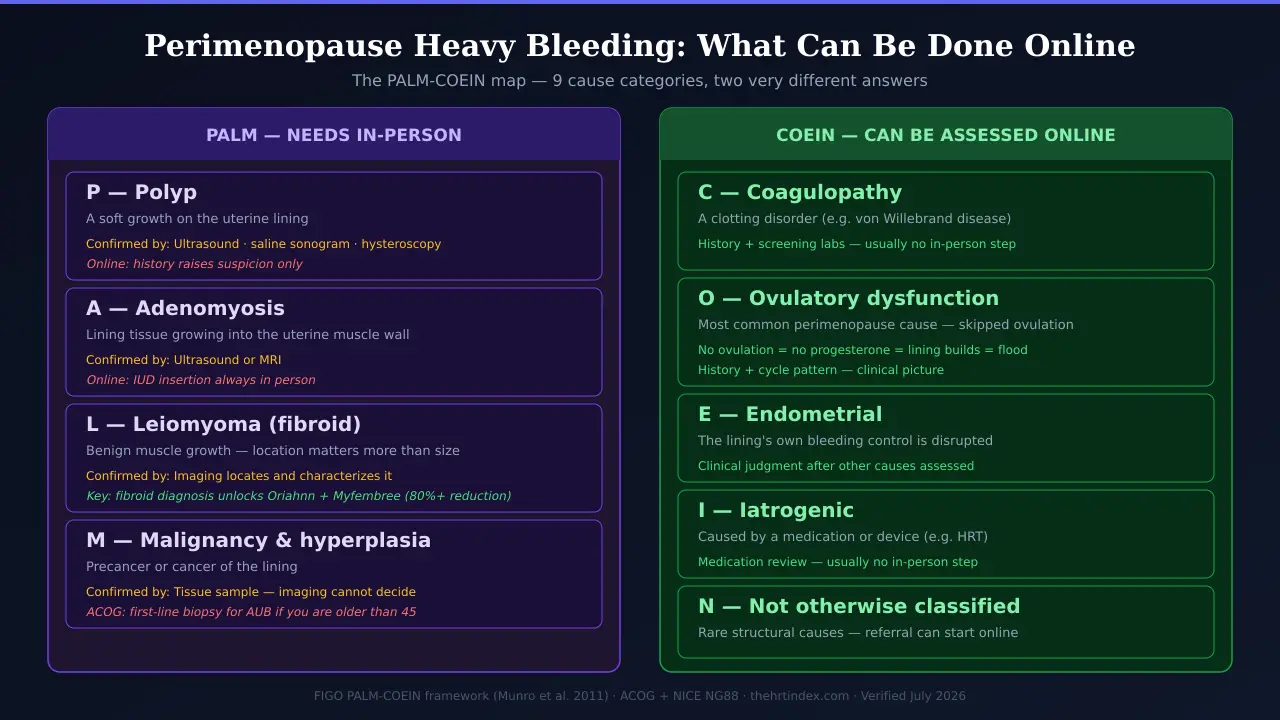
The PALM-COEIN Online-Care Map: nine cause categories for heavy perimenopausal bleeding, and where each one actually gets sorted out
Framework: Munro MG, Critchley HOD, Broder MS, Fraser IS; FIGO Working Group on Menstrual Disorders. Int J Gynaecol Obstet 2011;113:3–13. Evaluation per ACOG and NICE NG88. Verified July 2026.| Category | What it is | Can a virtual visit assess it? | What confirms it | What stays in person |
|---|
| P— Polyp | A soft growth in the lining | History can raise suspicion | Imaging— ultrasound, saline sonogram, or hysteroscopy | Imaging and any removal |
|---|
| A— Adenomyosis | Lining tissue growing into the muscle wall | History and exam can raise suspicion | Imaging— ultrasound or MRI | Imaging; IUD placement if that's the plan |
|---|
| L— Leiomyoma (fibroid) | Benign muscle growth. Where it sits matters more than its size | History can suggest a structural cause | Imaging locates and characterizes it | Imaging; procedures if needed |
|---|
| M— Malignancy & hyperplasia | Precancer or cancer of the lining | Risk assessment only | Tissue. Imaging can raise suspicion; histology decides | Sampling and treatment |
|---|
| C— Coagulopathy | A clotting disorder, like von Willebrand disease | ✓ Yes— history and screening labs | Blood testing; specialist input depends on findings | Usually nothing |
|---|
| O— Ovulatory dysfunction | A common cause in perimenopause.Skipped ovulation → unopposed estrogen → thick lining | ✓ Yes— history and pattern | Clinical picture, once other causes are assessed | Usually nothing |
|---|
| E— Endometrial | The lining's own bleeding control is off | Considered after other causes are assessed | Clinical judgment | Usually nothing |
|---|
| I— Iatrogenic | Caused by a medication or device | ✓ Yes— medication review | Medication history | Usually nothing → Bleeding after starting HRT |
|---|
| N— Not otherwise classified | Rare things, like a vascular malformation | Referral can start online | Specialist imaging | Testing and treatment |
|---|
Look at the pattern. Five of the nine categories can be worked up largely online. Four of them can't be settled anywhere but in a room with a machine or a microscope. Not “telehealth is useless.” Not “telehealth can do it all.” Five and four.
🎯 The FDA Label Map
We pulled the current FDA prescribing information for every medication labeled for heavy menstrual bleeding in the US. Not summaries. The labels. They don't agree with each other. And the way they disagree is the most useful fact on this page.
The FDA Label Map: six approved options for heavy menstrual bleeding, and the condition attached to each one
Source: FDA-approved prescribing information via accessdata.fda.gov and DailyMed, read July 2026.| Medication | What the label actually says | The condition attached |
|---|
Tranexamic acid
(generic Lysteda) | Cyclic heavy menstrual bleeding in females of reproductive potential | Section 2.1 is titled “Recommended Testing Prior to LYSTEDA Administration.” It says to exclude endometrial pathology first. Contraindicated with combined hormonal birth control. |
|---|
Natazia
(estradiol valerate/dienogest) | Heavy menstrual bleeding in women without organic pathology who choose an oral contraceptive | Requires that no identified organic cause is driving the bleeding. Boxed Warning. |
|---|
Mirena
(levonorgestrel IUS 52 mg) | Heavy menstrual bleeding for up to 5 years in women who choose intrauterine contraception | Tied to wanting an IUD. Requires a trained clinician to insert it. |
|---|
Liletta
(levonorgestrel IUS 52 mg) | Heavy menstrual bleeding in women who choose intrauterine contraception | Same structure as Mirena. In-person insertion. |
|---|
Oriahnn
(elagolix/estradiol/norethindrone) | Heavy menstrual bleeding associated with uterine fibroids in premenopausal women | Requires a diagnosed fibroid. Limited to 24 months because bone loss may continue and may not reverse. Boxed Warning. |
|---|
Myfembree
(relugolix/estradiol/norethindrone) | Heavy menstrual bleeding associated with uterine fibroids in premenopausal women | Requires a diagnosed fibroid. Limited to 24 months for the same reason. Boxed Warning. |
|---|
Read the right-hand column again
Natazia requires that you don't have fibroids. Oriahnn and Myfembree require that you do.
Tranexamic acid wants pathology excluded first. Mirena and Liletta want you to want an IUD.
Six labels. Six different conditions. Not one of them says “heavy bleeding, here's your pill.” And every single condition is something you cannot know from a questionnaire.
Go look for yourself: accessdata.fda.gov, search the drug name, read Section 1. It takes a minute.
Here's the part that should actually cheer you up
If your bleeding turns out to be caused by fibroids, you're not in worse shape. You're in better shape.
Oriahnn's manufacturer reports over 50% average bleeding reduction at month 12. Myfembree's phase 3 LIBERTY trials reported menstrual blood loss reductions of 82.0% and 84.3% from baseline at week 24. Those are big numbers. Bigger than anything else on this page.
And you cannot have either drug until somebody finds the fibroid. So the ultrasound isn't a hoop. For some women it's the key to the most effective medication available. It doesn't just rule things out. It can rule things in— and open a door that stays locked otherwise.
⚠️ Our damaging admission — and it's about us
If you came here hoping to buy an online hormone prescription tonight and be done, we think that's the wrong purchase. That's an awkward thing for a site that earns money when you book with hormone providers to say out loud. We're saying it because it's true and you'd find out the hard way.
Online menopause care does NOT include a pelvic exam, an ultrasound, a biopsy, or an IUD insertion. If what you need is a structural diagnosis, a virtual clinic can't finish that job.
But because a virtual visit doesn't require you to wait for a specialist's calendar, it's often the fastest way to get the workup moving. The clinician can assess the bleeding, start treatment if it's appropriate, and order the testing that fits your situation — so that by the time you see someone in person, you're walking in with results instead of starting from zero. That's not second best. That's a head start.
✓ So here's your first move
You need a clinician who can assess the bleeding and, when it's appropriate, order local imaging or route you to sampling. Sesame Careis a marketplace where you book directly with licensed clinicians — video orin person — at a cash price you see before you pay. It has an OB/GYN category, and clinicians there can order labs and imaging when clinically appropriate. BBB-accredited and LegitScript-certified.
Check for a Sesame clinician who evaluates abnormal uterine bleeding →Prices show before you book. Confirm the clinician you pick evaluates abnormal bleeding and coordinates local imaging. Sesame advertises general telehealth from around $34 — that's the all-specialty marketplace floor, not a gynecology price.
Before you click:if you're older than 45, if you've bled after 12 months without a period, or if someone has already told you that you need sampling — a virtual visit can help coordinate the handoff, but do not book a medication-only service expecting it to complete the in-person step.