This page is for you if:
- You started, restarted, or changed your menopause HRT, and now have spotting or bleeding
- You want to know what’s expected, what’s a warning sign, and who to call
- You’d like to walk into (or message) your appointment prepared
This page is NOT for you if:
- You have a positive pregnancy test or bleeding after miscarriage / surgery / a gynecologic procedure
- The blood might be from your bladder or bowel
- You’re bleeding hard right now and feel dizzy — see the emergency box
If pregnancy is possible and bleeding comes with one-sided lower-belly pain, shoulder-tip pain, marked dizziness, or fainting, seek urgent or emergency assessment. Those can be signs of an ectopic pregnancy. (Source: NHS.)
Start here: which situation are you in?
| What’s happening | What to do |
|---|---|
| Light early spotting, and you feel fine otherwise | Write it down and tell your prescriber |
| Bleeding that’s heavy, won’t stop, comes with pain, or starts after months of nothing | Book a prompt clinical check |
| Very heavy bleeding with dizziness, faintness, breathlessness, or chest pain | ⚠ Get emergency care — see box above |
Is bleeding after starting HRT normal?
Sometimes — but there is no single “normal” HRT bleed. A predictable monthly bleed is expected on cyclical HRT, while light unscheduled bleeding that fades over a few months can happen on continuous combined HRT. Whether your bleeding fits an expected pattern depends on your regimen, how long you’ve been on it, how much you’re bleeding, and whether you’d already stopped bleeding before. (Source: British Menopause Society, 2026; Mayo Clinic, 2025.)
Here’s the honest part most pages skip: “spotting is normal for the first six months” is true — and incomplete. The exact same spotting means one thing in a woman on a bleed-by-design regimen, and something very different in a woman who was postmenopausal, bleed-free, and suddenly isn’t. A blanket “wait it out” can accidentally talk someone out of getting a warning sign checked.
Three words your clinician uses, and what they mean:
| Type of bleeding | What it means | What to do with it |
|---|---|---|
| Scheduled (withdrawal) bleed | A bleed that arrives when it’s meant to — at the end of the progestogen days on a cyclical regimen | Expected by design; track timing and note any change |
| Unscheduled (breakthrough) bleed | Any bleed outside the pattern your regimen is built to produce | Often early settling; report it, and check it against the warning signs below |
| Postmenopausal bleeding | Bleeding 12+ months after your last natural period (different from a planned withdrawal bleed on cyclical HRT) | Always worth a call — even a small amount |
Progestogen is the umbrella term for progesterone (including the body-identical form) and synthetic versions called progestins — the hormone used to protect your uterine lining. (Source: BMS, 2026.)
What should you do right now if you start bleeding on HRT?
First, check for emergency symptoms. If there are none, don’t change your medication — figure out your regimen, note when you started or changed it, write down what the bleeding looks like, and contact your prescriber. Bleeding alone can’t tell you your dose is “too high” or your progesterone is “too low.” (Source: British Menopause Society, 2026.)
Four calm steps:
Rule out the red flags
Use the table below to decide how fast to move.
Confirm where the blood is coming from
Vaginal? Urinary? Rectal? Not sure? It matters — blood you notice after using the toilet isn't automatically from your uterus, and the source changes who you should see.
Find your medication
Note: your estrogen product and how you take it; your progesterone/progestogen product; whether you take it every day or only on certain days; your start date; your last change date; any missed doses. If it's a vaginal ring, write down the brand.
Don't diagnose the dose from the bleeding
Bleeding alone can't tell you which hormone to raise or lower. Changing it yourself — especially stopping the progestogen that protects your lining — can be the wrong move. Bring the facts to someone who can see the whole picture.
Step 1 in detail — how fast to move:
| Level | What it looks like | What to do |
|---|---|---|
| Emergency | Very heavy bleeding with faintness, dizziness, shortness of breath, chest pain, confusion, or severe weakness | ⚠ Emergency room or emergency services now |
| Same-day / urgent | Severe pelvic pain; fever; pregnancy possible with one-sided or shoulder-tip pain; rapidly worsening bleeding; or feeling suddenly unwell | Same-day clinician, urgent care, or a triage line |
| Prompt appointment | Flooding or repeated clots; bleeding lasting more than 7 days; light bleeding on most days for 4+ weeks; bleeding after sex; bleeding after months of none; or bleeding that starts more than 3 months after an HRT change | Your prescriber, a gynecologist, or primary care |
| Track & report | Light early spotting and you feel fine | Write it down and tell your prescriber |
Once the bleeding is handled, if your real challenge is finding good ongoing care for your menopause symptoms, that’s the moment for our matching tool.
Find My HRT Path → (free, ~90 seconds)Matches your state, insurance, regimen preference, and symptoms. Flags when in-person care is the right first step.
How does your HRT regimen change what the bleeding means?
Cyclical HRT is designed to give you a monthly bleed; continuous combined HRT is designed to eventually give you none; and low-dose vaginal estrogen isn’t meant to cause a uterine bleed at all. What matters most is whether your lining has proper protection and whether the bleeding matches what your specific regimen is built to do. (Source: Women’s Health Concern / BMS, 2026.)
| Your HRT type | What bleeding is expected | When it should settle | The pattern that means “get it checked” |
|---|---|---|---|
| Cyclical / sequential (estrogen daily, plus progestogen for ~10–14 days per cycle) | A predictable monthly bleed at the end of the progestogen days | Continues by design; extra early spotting often settles within ~6 months | Bleeding outside the scheduled window; withdrawal bleed lasting >7 days; flooding or clots; bleeding with pain or after sex |
| Continuous combined (“no-bleed”) | Unscheduled bleeding can occur early; long-term goal is no bleeding | Settling-in phase of up to six months is common | Bleeding that continues beyond six months, first begins later, or returns after a bleed-free stretch |
| Systemic estrogen, no separate lining protection (usually after total hysterectomy) | No uterine bleeding | n/a | Any vaginal bleeding — get the source checked |
| Low-dose vaginal estrogen (cream, ring, tablet) | Not meant to cause a uterine bleed | n/a | Any bleeding — don't assume it's "just dryness." See also: vaginal estrogen guide |
The one rule under all of this: lining protection
If you have a uterus and take systemic estrogen, your lining needs protection from a progestogen — otherwise estrogen can build the lining up over time and raise the risk of overgrowth (hyperplasia) and cancer. That protection can come as a combined product, a separate progesterone, or a supported 52 mg levonorgestrel IUD. Never add, cut, or stop that protection on your own — call your prescriber. (Source: The Menopause Society; FDA.)
Cyclical (sequential) HRT
You take estrogen steadily and add progestogen for part of each cycle, which triggers a planned bleed when it drops. The questions that matter: Is this bleed on schedule? Is it heavier or longer than before? On-schedule and steady is usually the plan working. Off-schedule, flooding, clots, or a bleed lasting more than seven days is worth a call.
Continuous combined HRT
You take both hormones every day, and the long-term goal is no bleeding. Early spotting while your lining settles is common — a settling-in phase of up to six months. What’s not in the “just settling” category: bleeding that starts up again after you’d gone quiet, or bleeding still going strong past six months. That earns a review.
Are all estrogen vaginal rings local? No — and this trips people up.
Estring is a low-dose, local ring: it releases about 7.5 micrograms of estradiol a day to treat vaginal symptoms only, with very little reaching the rest of your body. Femring is a systemic ring: it releases a much higher dose and treats whole-body symptoms like hot flashes — which means, if you have a uterus, your lining still needs protection. So "I'm on a vaginal ring" isn't enough information. Write down the brand. (Source: FDA labeling for Estring and Femring.)
Which hormonal IUD can protect the uterine lining during HRT?
A 52 mg levonorgestrel IUD (such as Mirena) may be used as the progestogen part of an HRT regimen. Lower-dose hormonal IUDs don't have the same evidence for protecting the lining, so they aren't interchangeable. One important US note: using a 52 mg levonorgestrel IUD as the progestogen component of menopause HRT is off-label in the US — worth understanding. Early spotting can also have more than one source when an IUD is involved, so note your IUD type and insertion date. (Source: BMS, 2026; FDA / Mirena labeling.)
If you're only on low-dose vaginal estrogen
Local vaginal estrogen isn't meant to cause a uterine bleed, and its labeling does note that irregular spotting can occasionally happen. But here's the rule we won't bend: unexplained bleeding after menopause should not be waved off as "vaginal dryness." Call your prescriber, especially if it comes back or follows sex. (Source: FDA labeling.)
What if I had a subtotal hysterectomy or endometrial ablation?
Confirm exactly which operation you had before assuming your lining needs no protection. A subtotal (partial) hysterectomy can leave a small amount of uterine-lining tissue behind, and endometrial ablation doesn't reliably remove every part of the lining — so bleeding is still possible and still worth checking. A history of severe endometriosis can also change the recommended regimen after hysterectomy. If any of these is you, don't assume; ask. (Source: BMS, 2026.)
How long can bleeding after starting HRT last?
Light, irregular bleeding can come and go for the first several months and often settles within about six months — but the calendar isn’t a license to wait through every kind of bleeding. Bleeding that’s heavy, that starts long after you began, or that shows up after you’d stopped bleeding deserves an earlier look. (Source: British Menopause Society, 2026; Mayo Clinic, 2025.)
| Time since started HRT | Time since last change | Were you bleed-free before? | What it suggests | What to do |
|---|---|---|---|---|
| First few months | — | You'd never settled | Common early adjustment | Track it; tell your prescriber |
| — | Within 3 months of a change | Recently stable | Can fall within an adjustment window | Note the exact change; contact prescriber; don't self-adjust |
| More than 6 months | — | Had settled, now bleeding again | Beyond a simple settling phase | Prompt clinical assessment |
| — | More than 3 months after a change (new bleed) | Recently stable | Treated differently — not just 'adjustment' | Prompt clinical assessment |
| Any | Any | Bleed-free for months, now bleeding | A new event, not leftover from starting | Prompt clinical assessment |
The pattern to remember: time matters, but amount, symptoms, and whether you’d already gone quiet matter more. A heavy, painful bleed at week three is more urgent than a fleck of spotting at month five.
When does bleeding after HRT need prompt or urgent evaluation?
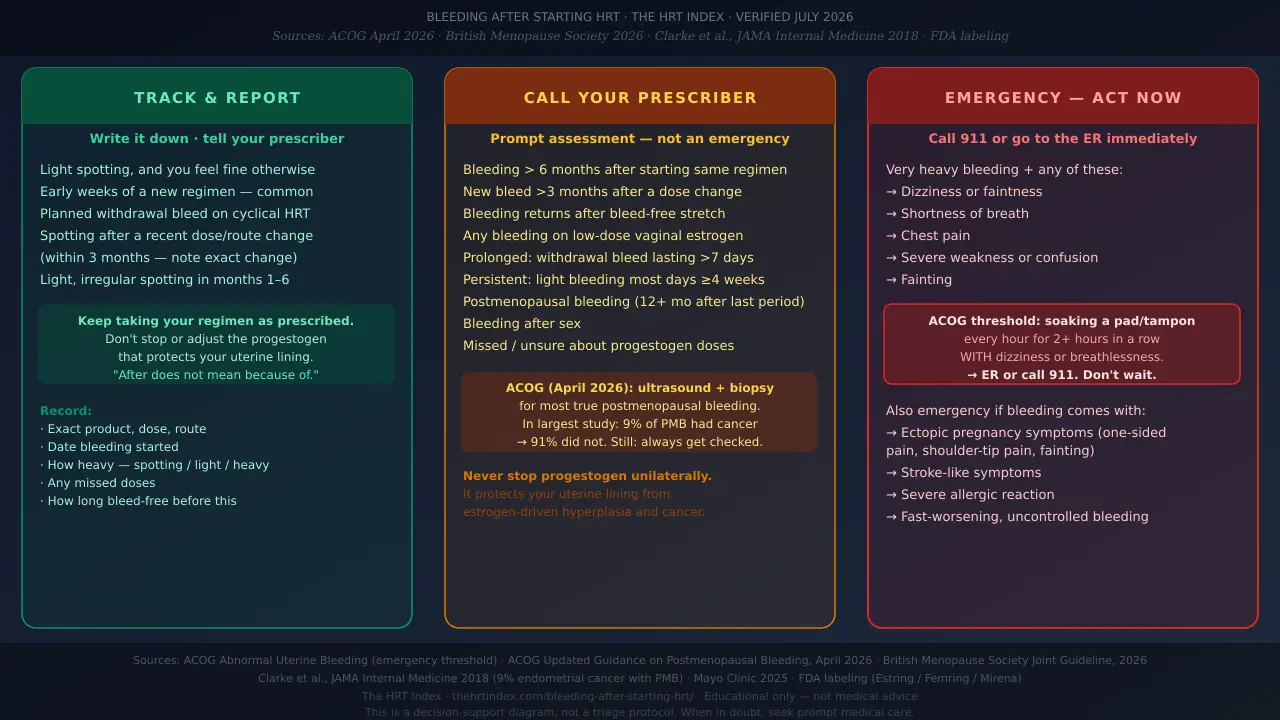
Call a clinician promptly if your bleeding is heavy, lasts more than a week, happens after sex, returns after a bleed-free stretch, or occurs 12+ months after your last natural period. Very heavy bleeding with dizziness, faintness, chest pain, or breathlessness is an emergency. (Source: British Menopause Society, 2026; ACOG, 2026.)
First, pinning down the words this page keeps using — from the 2026 BMS guideline:
| Term | What it actually means |
|---|---|
| Prolonged | A withdrawal bleed lasting more than 7 days |
| Heavy | Flooding and/or clots |
| Persistent | Even light bleeding that happens on most days for 4 weeks or more |
The HRT Index Bleeding-After-HRT Action Matrix
Last verified · Editorial synthesis, not a diagnosis. Action level is based on your regimen, time since starting or changing HRT, prior bleed-free interval, bleeding amount and duration, associated symptoms, pregnancy possibility, and endometrial-risk context.
| Your situation | What it may mean (not a diagnosis) | Safest next step | Basis |
|---|---|---|---|
| Cyclical HRT, predictable bleed at the end of the progestogen days | A scheduled withdrawal bleed — likely the regimen working | Track timing and flow; flag any change | BMS (UK) |
| Continuous combined HRT, light spotting in the first 6 months | Early settling — but this type is meant to become bleed-free | Report it and track it, don't just assume it's harmless | BMS (UK); Mayo (US) |
| Bleeding within 3 months of a dose/route/product change | Possibly tied to the change | Contact prescriber; note the exact change; don't self-adjust | BMS (UK) |
| A new bleed first starting more than 3 months after a change | Handled differently than early adjustment | Prompt clinical assessment | BMS (UK) |
| First bleeding more than 6 months after starting the same regimen | Less like early settling | Prompt clinical assessment | BMS (UK) |
| Bleeding returns after months of being bleed-free | A new change — don't blame HRT by default | Prompt clinical assessment | BMS (UK); Mayo (US) |
| Prolonged (>7 days), heavy (flooding/clots), or persistent (light most days for 4+ weeks) bleeding | Reasons to check for a lining problem | Prompt clinical assessment; escalate if you feel unwell | BMS (UK) |
| Soaking a pad/tampon hourly for 2+ hours with dizziness or breathlessness | Possible significant blood loss | ⚠ Emergency care | ACOG (US) |
| Any new bleeding 12+ months after your last natural period | Postmenopausal bleeding — always worth checking | Report it and arrange evaluation | ACOG (US); Mayo (US) |
| You have a uterus, use systemic estrogen, and missed or aren't sure about the progestogen | Your lining's protection may need prompt review | Contact prescriber; don't stop or cut the progestogen yourself | BMS (UK); The Menopause Society |
| You might still be perimenopausal, or pregnancy is possible | Natural cycles can continue; HRT is not birth control | Consider a pregnancy test if relevant; contact prescriber | NHS (UK); The Menopause Society |
| Bleeding after sex, with pain, unusual discharge, or an unclear source | May come from the vagina, cervix, uterus, bladder, or bowel | Get it assessed so the source is identified | ACOG (US); Mayo (US) |
| Bleeding while using low-dose vaginal estrogen | Local irritation is possible — but don't assume that's all | Contact prescriber or a gynecologic clinician | FDA labeling |
A note for US readers: Some of the most detailed guidance comes from the UK’s BMS. It’s excellent — but it uses UK-specific referral timelines and ultrasound-measurement cutoffs that we’ve deliberately not turned into US self-diagnosis numbers. Use the matrix to know when to reach out; let your clinician decide the how.
Why can HRT cause bleeding in the first place?
HRT changes how your uterine lining responds to estrogen and progestogen, and on cyclical regimens the drop in progestogen is meant to cause a bleed. Bleeding can also come from missed doses, a recent change in your regimen, natural perimenopausal cycles, vaginal or cervical changes, polyps, fibroids, infection, or — less often — a thickened lining or cancer. Timing alone can’t tell you which. (Source: BMS, 2026; Mayo Clinic, 2025.)
Common, benign reasons
- Lining settling into a new hormone balance — the usual story in the first few months
- A planned withdrawal bleed on cyclical HRT
- Missed or late doses — skipping a patch, gel, pill, or progesterone dose can throw off the pattern
- A recent change — a new dose, route, or product
- Natural perimenopause — your ovaries may still be doing their own thing
Reasons unrelated to HRT — why it can’t be brushed off
- Thinning, delicate vaginal or cervical tissue
- Polyps or fibroids
- Infection
- A thickened uterine lining (hyperplasia)
- Endometrial (uterine) cancer
- Blood from the bladder or bowel
Mayo Clinic lists tissue thinning, polyps, infection, hyperplasia, and endometrial cancer among possible causes of bleeding after menopause. The point isn’t to scare you — most of these are benign or very treatable — it’s that you can’t sort them by color or gut feeling.
A straight word on compounded vs. FDA-approved HRT
Compounded drugs are not FDA-approved. The FDA does not review their safety, effectiveness, or quality before they’re marketed. BMS warns that compounded transdermal progesterone creams and gels can absorb unpredictably and may not provide enough protection for the uterine lining — which is directly relevant if you’re bleeding on that kind of product. Compounded HRT is not the same as, safer than, or more “natural” than FDA-approved HRT. (Source: FDA; BMS, 2026.)
Does bleeding after starting HRT mean cancer?
No — bleeding does not mean you have cancer, and most postmenopausal-bleeding episodes are not caused by endometrial cancer. In the largest study of its kind, 9% of women with postmenopausal bleeding were found to have endometrial cancer — which means about 91% were not — and the risk was even lower among women on hormone therapy. (Source: Clarke et al., JAMA Internal Medicine, 2018.)
We’re deliberately not going to tell you “it’s probably nothing.” Your personal odds can’t be read from blood color, a single photo, how heavy it is, one missed dose, or the fact that you just started HRT. “Probably nothing” is a population statement. You’re a person. The grown-up move is to get the reassurance confirmed rather than assumed.
| Group studied | Share with endometrial cancer | Does this apply directly to your early HRT spotting? |
|---|---|---|
| All women with postmenopausal bleeding | 9% | No — a population estimate, not your personal risk |
| Women in North American studies | 5% | No — population estimate only |
| Women who were on hormone therapy | ~7% | No — but it points the same way: HRT users sat lower, not higher |
A scan or biopsy is an investigation, not a diagnosis
Being sent for a transvaginal ultrasound or a lining biopsy means your doctor is checking things in the right setting — it does not mean anything has been found. Most women who have these tests turn out not to have cancer.
When it is found, it’s usually caught early
About 91% of women diagnosed with endometrial cancer had postmenopausal bleeding first. Reporting a bleed is one of the most reliable early-warning signals in women’s health — a reason to act rather than panic.
What will your doctor ask — and what should you record?
The most useful things to bring are your bleeding pattern and amount, when you started HRT, exactly what you take and how consistently, how long you’d been bleed-free before, and your relevant risk history. (Source: BMS, 2026.)
The minimum useful record
- HRT start date and most recent change date
- Your exact estrogen product and route
- Your exact progesterone/progestogen product
- Whether it’s continuous or cyclical
- Whether you have a uterus (and any uterine surgery)
- The date bleeding started and each day it’s happened
- How heavy: spotting / light / period-like / heavy (flooding/clots)
- Prolonged (>7 days) or persistent (most days for 4+ weeks)
- Pelvic pain, bleeding after sex, or faint/breathless
- Any missed doses
- Date of last natural period and how long bleed-free
- Whether pregnancy is possible
Ten questions worth asking at the visit
- Is this bleeding expected for my exact regimen?
- Does the timing change whether it should be investigated?
- Do I need an exam, ultrasound, or biopsy?
- Is my lining protected correctly for my situation?
- Should I keep taking my regimen unchanged while I wait?
- What amount or symptom would mean I need urgent care?
- When should I follow up if it continues?
- Could the blood be from my vagina, cervix, bladder, or bowel?
- Is a pregnancy test relevant for me?
- What should I track between now and then?
Copy-and-paste message for your patient portal
“I started [HRT product/regimen] on [date] and last changed [dose/route/product] on [date]. Bleeding began on [date]. It’s been [spotting / light / period-like / heavy] on [number] days. Before this I’d been bleed-free for [interval]. Other symptoms: [list]. I have / have not missed doses. Do I need an exam or imaging, and should I keep taking my regimen exactly as prescribed while I wait?”
Risk factors worth mentioning if they apply (your clinician uses these to decide how fast to move): known Lynch or Cowden syndrome, or a strong personal or family history of endometrial or colorectal cancer; a BMI of 40 or higher; diabetes, PCOS, or a BMI of 30–39; and any stretch of taking estrogen without adequate lining protection. These are factors, not a home cancer score — don’t try to calculate your own risk from them. (Source: BMS, 2026.)
What tests might be recommended for bleeding on HRT?
Evaluation may include your history, a physical and pelvic exam, a pregnancy test if relevant, a transvaginal ultrasound, and sometimes an endometrial biopsy or hysteroscopy. The right order depends on your age, regimen, bleeding pattern, risk history, and where you live. (Source: ACOG, 2026; BMS, 2026.)
Your clinician asks about your exact regimen, how consistently you take it, your dates, and your risk factors. This isn't nosiness — it changes the plan.
May include checking your cervix and vagina, cervical screening if you're due, and testing for infection if it fits.
Only if pregnancy is possible. Worth repeating: menopause HRT is not birth control, and you can still conceive during perimenopause.
A wand-style scan that looks at your uterus and the thickness of your lining, and can spot polyps or fibroids. Don't try to interpret a single measurement on your own — the number only means something in the context your clinician adds.
A small sample of the lining, usually taken in the office. Being offered one does NOT mean cancer was found — it's how the lining gets checked directly.
A thin camera used to look inside the uterus, often to find a specific cause like a polyp.
What changed in ACOG’s 2026 guidance?
In , ACOG updated its guidance on evaluating postmenopausal bleeding. ACOG now recommends both a transvaginal ultrasound and endometrial tissue sampling as part of the initial evaluation for most patients with postmenopausal bleeding — because ultrasound alone can miss an estimated 5–12% of cancers.
Ultrasound alone may be considered only for a selectpatient: one with a single bleeding episode, a fully visualized lining measuring 4 mm or less, no strong endometrial-cancer risk factors, reliable access to prompt gynecologic care, and clear counseling that any continued or recurrent bleeding needs immediate reassessment. In other words, a thin lining is one part of a narrow exception — the measurement alone doesn’t make a biopsy unnecessary for most patients under the 2026 guidance.
Does ACOG’s 2026 biopsy recommendation apply to early HRT spotting? Not automatically. That recommendation is about true postmenopausal bleeding — bleeding presumed to come from the uterus at least 12 months after your final period — not light spotting in your first months on HRT. If you’re a few weeks into a new regimen with some spotting and you feel fine, your clinician may reasonably watch, adjust, and reassess rather than jump straight to a biopsy. The clinical picture drives it. (Source: ACOG, 2026; BMS, 2026.)
US vs. UK evaluation, side by side
| Situation | US approach (ACOG, 2026) | UK approach (BMS, 2026) | What you do |
|---|---|---|---|
| True postmenopausal bleeding (12+ months after final period) | Ultrasound plus biopsy for most patients | Assess, ultrasound pathway, referral by risk and pattern | Report promptly; expect evaluation |
| Early unscheduled bleeding on HRT | Judged on the clinical picture; not an automatic biopsy | 'Settling-in' window recognized; adjust and reassess | Track it; contact your prescriber |
| Heavy, prolonged, or persistent bleeding | Prompt evaluation | Urgent ultrasound pathway (UK-specific timing) | Prompt clinical contact; escalate if unwell |
Should you stop or change HRT because of bleeding?
No — don’t use bleeding alone to decide your dose is too high or to redesign your regimen yourself. If you have a uterus, quietly stopping the progestogen that protects your lining can be exactly the wrong move. (Source: BMS, 2026.)
What a clinician might review or adjust: missed doses, patch or gel technique, whether you’re on the right continuous-vs-cyclical schedule, your estrogen dose and route, your progestogen product and timing, or adding a progestogen-releasing IUD for lining protection. BMS specifically allows progestogen or HRT adjustments while assessment is pending— so “we’re looking into the bleeding” and “let’s tweak your regimen” aren’t mutually exclusive.
The honest tradeoff: HRT might be doing a wonderful job on your hot flashes, sleep, or mood whilethe bleeding is driving you up the wall. Both things can be true at once, and you don’t have to pretend one cancels the other. If your doctor says the pattern is unlikely to be dangerous but you still can’t live with the bleeding, that is a completely valid reason to ask for a management change. You’re allowed to ask for a clearer answer than “that’s normal.”
For the full picture on side effects beyond bleeding, see: HRT side effects overview · progesterone side effects in menopause · micronized progesterone side effects.
What if you’re still in perimenopause, or pregnancy is possible?
Natural cycles can keep going during perimenopause, and HRT does not work as contraception. If pregnancy is possible, a pregnancy test and a chat with your clinician may be worthwhile. (Source: NHS, 2026.)
Two things to hold onto. First, if you’re perimenopausal, some of your bleeding might be your own cycle and some might be HRT settling — and no article can reliably separate the two for you. Second, HRT is not birth control. If you could still become pregnant, your contraception is a separate conversation.
If pregnancy is possible and the pain is one-sided: one-sided lower-belly pain, shoulder-tip pain, marked dizziness, or fainting — especially with bleeding — can be signs of an ectopic pregnancy, which is a medical emergency. Don’t wait it out; seek urgent or emergency assessment. (Source: NHS.)
What we actually verified for this guide
| What we state | Source | Date | Where it applies |
|---|---|---|---|
| Emergency threshold for very heavy bleeding | ACOG, Abnormal Uterine Bleeding | Current | US |
| Ultrasound + biopsy for most postmenopausal bleeding | ACOG, updated guidance on evaluating postmenopausal bleeding | April 2026 | US |
| Endometrial-cancer risk with PMB (9% overall; ~5% North America; ~7% HT users; ~91% of cancers had PMB) | Clarke et al., JAMA Internal Medicine | 2018 | International (incl. US) |
| Definitions of prolonged / heavy / persistent bleeding; settling-in window; lining protection | British Menopause Society joint guideline | 2026 | UK (labeled) |
| Uterus + systemic estrogen needs progestogen protection | The Menopause Society | Current | North America |
| Bleeding causes after menopause | Mayo Clinic | 2025 | US |
| Estring is local; Femring is systemic; Mirena's US indications | FDA labeling | Current | US |
| HRT is not contraception | NHS | 2026 | UK (general principle) |
Last verified: using The HRT Index Verification Standard. Research by The HRT Index Editorial Team — editorial research, not reviewed by a clinician, not medical advice. Spot something out of date? Tell our editorial team — we date any material correction.
Frequently asked questions about bleeding after starting HRT
Short answers to the follow-up questions women search most — same rule throughout: your regimen, timing, amount, prior stability, and other symptoms decide the next step.
What should you do next?
If you have emergency symptoms
Get emergency medical care now. Call 911 or go to the ER. Don't stop to fill out a tool first.
If your bleeding is heavy, prolonged, persistent, postmenopausal, after sex, painful, or new after a stable stretch
Contact a gynecologic, primary-care, urgent-care, or prescribing clinician.
If it's light early spotting and you feel fine
Write it down, keep taking your regimen as prescribed, and tell your prescriber.
If the bleeding's sorted and you now need ongoing HRT care that fits you
Use The HRT Index's Find My HRT Path tool to match your state, insurance, medication preferences, and symptoms — and to flag when you'd be better off with an in-person clinician first.
Still not sure which HRT path fits?
Take the free 90-second Find My HRT Path quiz for a best-fit care route and two backup options. We built it to help you skip the trial-and-error and land with care that fits your situation before you spend a dollar or sit through a consult that was never going to work for you.
Start the quiz →Free. No email required. No provider pushed on you. If the quiz suggests providers, any affiliate links are labeled and rankings aren’t sold.
Sources
All sources reviewed July 2026. Every claim is paraphrased; no source text is reproduced.
- American College of Obstetricians and Gynecologists (ACOG). Updated Guidance on the Evaluation of Postmenopausal Bleeding. April 2026.
- ACOG. Abnormal Uterine Bleeding (patient FAQ — emergency threshold).
- Clarke MA, Long BJ, Del Mar Morillo A, et al. Association of Endometrial Cancer Risk With Postmenopausal Bleeding in Women: A Systematic Review and Meta-analysis. JAMA Internal Medicine. 2018;178(9):1210–1222.
- British Menopause Society, with RCOG, BGCS, BSGE, FSRH, RCGP, and GIRFT. Management of Unscheduled Bleeding on HRT (joint guideline). Reviewed 2026. thebms.org.uk
- Women’s Health Concern / British Menopause Society. Management of Unscheduled Bleeding on HRT (patient factsheet). Reviewed 2026.
- The Menopause Society. Hormone Therapy (patient education — uterus and progestogen). menopause.org
- Mayo Clinic Press. What causes bleeding after menopause? December 2025.
- Cleveland Clinic. Postmenopausal Bleeding: Causes, Diagnosis & Treatment. Updated January 15, 2024.
- U.S. Food and Drug Administration. Compounding and the FDA: Questions and Answers; prescribing information for Estring and Femring; Mirena prescribing information.
- NHS. Menopause and perimenopause — symptoms; HRT and contraception; Ectopic pregnancy — symptoms. Reviewed 2026.
Update history
— Published. Verified ACOG April 2026 postmenopausal bleeding guidance; BMS 2026 joint guideline; Clarke et al. 2018 meta-analysis; FDA labeling (Estring, Femring, Mirena); NHS ectopic pregnancy guidance.
This guide is editorial research and is not medical advice. It was not reviewed by a clinician. Always talk with the professional who manages your HRT before making changes. Emergency symptoms need emergency care — don’t wait.