This page is for you if:
- You were prescribed micronized progesterone (Prometrium or a generic) for menopause HRT or missed periods
- Your bottle says “progesterone,” “micronized progesterone,” or “Prometrium”
- You’re figuring out whether a symptom is normal or needs action
Stop and get help now if:
- Chest pain, sudden shortness of breath, swollen or painful leg, sudden severe headache, trouble speaking or seeing — call 911
- Peanut allergy and your Prometrium product hasn’t been confirmed — call your prescriber or pharmacist before your first dose
The 10-second version
| What you’re noticing | First take | What to do |
|---|---|---|
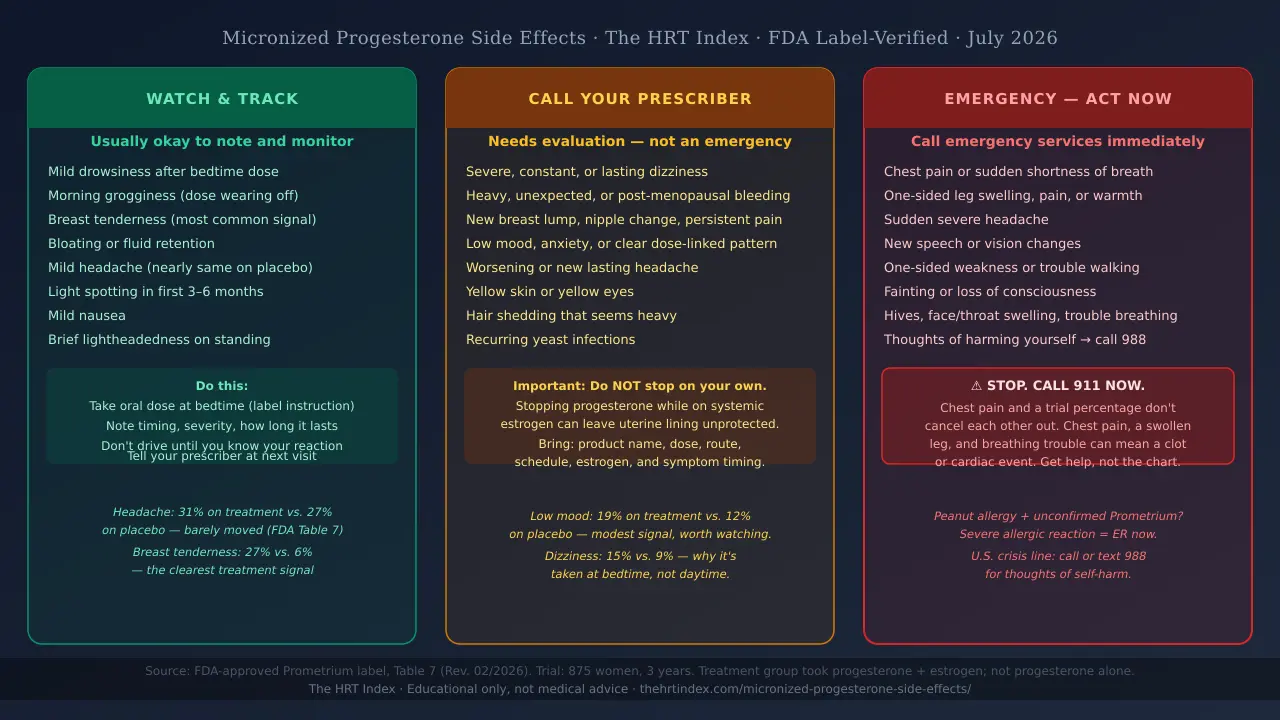
| Mild drowsiness, breast tenderness, bloating, nausea, or light spotting | Usually okay to watch | Follow your product’s instructions (oral Prometrium is taken at bedtime). Track when it happens and how bad it is. |
| Severe or lasting symptoms, worsening mood, or unexpected bleeding | Call your prescriber | Don’t change or stop your dose on your own. |
| Chest pain, sudden trouble breathing, one-sided leg swelling, stroke-like signs, fainting, or a severe allergic reaction | Emergency | ⚠ Call your local emergency number now. |
The full, sourced version is below. One honest limitation: the clearest side-effect numbers come from a trial where women took micronized progesterone togetherwith estrogen — not progesterone alone. So the numbers can’t perfectly separate what progesterone did from what estrogen did.
What are the most common micronized progesterone side effects?
The side effects reported most often are headache, breast tenderness, low mood, dizziness, and bloating. But when you place those numbers next to a placebo group, the picture changes: breast tenderness clearly rose with treatment, while headache happened nearly as often on a dummy pill. Most effects are mild and ease as your body settles in.
Micronized progesterone is progesterone ground into tiny particles so your body can absorb it better. It’s made in a lab from a plant source, but it’s chemically identical to the progesterone your own body makes— which is why it’s often called “body-identical.”
The clearest U.S. numbers come from the FDA-approved Prometrium label — specifically Table 7, which shows two groups inside an 875-woman, three-year study: 178 women took 200 mg of Prometrium (12 days each cycle) plus conjugated estrogen, and 174 women took a placebo.
FDA Table 7 — Reported effects with context
| Reported effect | On progesterone + estrogen | On placebo | What the difference tells us |
|---|---|---|---|
| Breast tenderness | 27% | 6% | The clearest signal. Rose sharply with treatment (estrogen adds to this too). |
| Depression / low mood | 19% | 12% | Reported more with treatment. A modest signal worth watching. |
| Joint pain | 20% | 29% | Reported less often with treatment than placebo. |
| Dizziness | 15% | 9% | Rose with treatment — part of why it's taken at bedtime. |
| Bloating | 12% | 5% | Rose with treatment. |
| Hot flashes | 11% | 35% | Far fewer with treatment — the estrogen is treating them. |
| Vaginal discharge | 10% | 3% | Rose with treatment. |
| Abdominal pain | 10% | 10% | Same on both — not a treatment effect. |
| Nausea / vomiting | 8% | 7% | About the same on both. |
| Night sweats | 7% | 17% | Far fewer with treatment — the estrogen is treating them. |
| Headache | 31% | 27% | Barely moved. Nearly as common on a placebo. |
| Urinary problems | 11% | 9% | About the same on both. |
| Worry | 8% | 4% | Reported a bit more with treatment. |
| Chest pain | 7% | 5% | Reported slightly more — chest pain is never 'just a side effect' (see safety note below). |
| Diarrhea | 7% | 4% | Reported a bit more with treatment. |
| Breast pain | 6% | 2% | Reported more with treatment. |
| Swelling of hands/feet | 6% | 9% | Reported less often with treatment. |
| Vaginal dryness | 6% | 10% | Reported less often with treatment. |
| Constipation | 3% | 2% | About the same on both. |
Read that table once and the whole topic gets calmer.The symptom people dread most — headache — barely moved (31% vs 27%). The effect that clearly rose with treatment is breast tenderness. And “menopause” symptoms like hot flashes went down, because the therapy is treating them.
Three more rows, kept honest
The same trial recorded three uncommon events at 2% each (versus under 1% on placebo): breast carcinoma, a breast biopsy, and gallbladder removal (cholecystectomy). Small-number findings in one 178-woman group — not established rates. The breast-cancer question gets the fuller answer below.
Two things the patient label also lists as common:hair loss and vaginal yeast infections. Neither is dangerous on its own, but if hair shedding is heavy or a yeast infection won’t clear, tell your prescriber.
Why “reported” doesn’t mean “the progesterone caused it”: the trial mixed progesterone with estrogen, menopause symptoms come and go on their own, and other medicines or poor sleep can pile on. Treat any single symptom as a clue, not a verdict.
The right online HRT provider isn’t the same for every woman — it depends on your symptoms, your age and whether you have a uterus, your medication route, your risk history, your insurance or cash-pay situation, and your state.
Find My HRT Path → (free, ~90 seconds)Which micronized progesterone side effects are dangerous — and when do I call?
Get emergency help for chest pain, sudden shortness of breath, a swollen or painful leg, a sudden severe headache, new speech or vision changes, one-sided weakness, fainting, or a severe allergic reaction. Call your prescriber promptly about milder symptoms that last or worry you.
One safety note: some symptoms — like sudden vision changes, slurred speech, or trouble walking — can be signs of a stroke or clot. Those are emergencies, even though milder grogginess is not. When in doubt, treat the sudden or severe version as an emergency.
| Symptom or situation | Usually watch and record | Call your prescriber promptly | Get emergency help now |
|---|---|---|---|
| Mild drowsiness or dizziness | Follow bedtime instructions; don't drive while affected | If it's severe, constant, or stops you functioning | If you faint, can't stay awake, or have trouble breathing |
| "Drunk," disoriented, or very unsteady feeling | — (not a 'wait and see' symptom when strong) | Yes — right away | Loss of consciousness, major speech or movement trouble, breathing trouble |
| Headache | Mild and short: note the pattern | New, lasting, worsening, or migraine-like | Sudden severe headache, or headache with weakness, speech, vision, or balance changes |
| Breast tenderness | Note how bad and how long | A new lump, nipple change, or pain that won't quit | Not usually an emergency on its own |
| Bloating, cramps, nausea | Mild is fine to track | Severe, dehydrating, or repeated vomiting | If paired with chest, breathing, or collapse symptoms |
| Spotting or bleeding | Record date, amount, and cycle position | Heavy, after menopause, new after months of calm, or won't settle | Severe bleeding with faintness or collapse |
| Low mood, anxiety, irritability | Note timing vs. your dose | New, lasting, or worsening | Thoughts of harming yourself — get help now (call or text 988) |
| Puffiness / fluid retention | Note it; don't assume it's fat gain | Lasting or worsening swelling on both sides | One-sided painful leg swelling, chest pain, or shortness of breath |
| Yellow skin or eyes | — (don't just monitor this) | Yes, promptly | With confusion, severe illness, or collapse |
| Hives, face or throat swelling, trouble swallowing | — | — | Emergency now |
| Chest pain or sudden shortness of breath | Never treat as 'just a side effect' | — | Emergency now |
| One-sided leg pain, warmth, or swelling | Never treat as ordinary fluid retention | — | Emergency now |
A word on chest pain. You’ll notice chest pain sits in the data table at 7% (vs. 5% on placebo). That does not make chest pain a normal side effect to shrug off. A symptom can show up in a trial and still be an emergency in real life. Chest pain, a swollen leg, and trouble breathing can be signs of a blood clot or a heart problem. When those hit, the trial percentage is irrelevant — get help.
If you’re having thoughts of harming yourself, you’re not alone, and it’s not something to “wait out.” In the U.S., call or text 988(the Suicide & Crisis Lifeline), or go to your nearest emergency room. Mood changes are a recognized effect worth taking seriously.
Who should not take Prometrium?
The current FDA-approved Prometrium label says you should not take it if you have a peanut allergy, unexplained vaginal bleeding, a current or past breast cancer, a current or past blood clot in the legs or lungs, a current or past stroke or heart attack, or liver disease. It also should not be used during pregnancy.
Straight from the label, Prometrium is contraindicated(a medical word for “should not be used”) if you have any of these:
This list isn’t about scaring you — it’s the short set of situations where the risks clearly outweigh the benefits, and where your prescriber needs to know before you start.
Why does micronized progesterone make me tired, dizzy, or “hungover”?
Drowsiness and dizziness are recognized effects of oral micronized progesterone. Your liver breaks it down into calming byproducts (including allopregnanolone), and the label specifically warns it can make you drowsy or dizzy — which is why oral Prometrium is taken at bedtime.
Lots of women describe the next morning as feeling foggy, groggy, or “hungover.” That’s a common way to describe the bedtime dose still wearing off. The label doesn’t put a number on how often that happens, so we won’t invent one — but taking it at night is the point: you sleep through the heavy part.
| Usually okay to track | Not something to push through |
|---|---|
| Sleepiness after the bedtime dose | Extreme or long-lasting inability to function |
| Mild morning grogginess | Blurred vision |
| Brief lightheadedness when you stand up | Slurred speech |
| Mild dizziness with no other warning signs | Trouble walking, fainting, or breathing trouble |
Don’t drive, bike in traffic, or run machinery while you feel dizzy, groggy, or foggy. Wait until you know your reaction.
Food changes absorption. The label notes that taking oral Prometrium with food raised the amount absorbed in postmenopausal women given the 200 mg dose. Follow your own prescription the same way each night, and ask your pharmacist before changing your food timing.
How long do micronized progesterone side effects last?
There’s no single deadline by which every effect should vanish. Mild effects often ease over the first weeks as your body adjusts. But severe symptoms, unsafe grogginess, heavy or surprise bleeding, or anything that disrupts your life should prompt a check-in — not a wait.
| When | What to expect |
|---|---|
| After the first dose | Drowsiness or dizziness can show up fast. Check safety first. |
| First few days | Note how consistent, how strong, and whether it affects your daytime. |
| First few weeks | Mild headache, breast tenderness, or stomach symptoms may ease. If they don't, that's worth a call. |
| First 3–6 months of HRT | Bleeding and spotting are common while your body adjusts. Heavy or unexpected bleeding still needs a look. |
| Any time | Emergency warning signs are never 'waited out.' |
Symptoms that never get an “adjustment period”: chest pain, sudden shortness of breath, one-sided leg swelling, stroke-like changes, fainting, a severe allergic reaction, or thoughts of self-harm. Those get help, not patience.
Does micronized progesterone cause weight gain or bloating?
The label doesn’t establish that oral micronized progesterone causes lasting fat gain. It lists fluid retention as a common effect. After-market reports include both weight increases and decreases — reports that can’t prove how often something happens or what caused it. The Menopause Society says menopause hormone therapy overall isn’t linked to weight gain.
Bloating — That puffy, full feeling.
Fluid retention — Your body holding onto water. The label lists this as a common effect.
A number change on the scale — Can be water, not fat.
Actual body-fat gain — Not established for this medication.
When swelling is NOT ordinary bloating: mild puffiness on both sides is usually fluid — note it. But one-sided painful or warm leg swelling, or swelling with chest pain or shortness of breath, is an emergency. That can be a clot.
Can micronized progesterone cause depression, anxiety, or mood changes?
Mood can go either way. Some women feel steadier; others notice low mood or irritability. In the trial, low mood was reported by 19% on treatment vs. 12% on placebo — a modest difference, and those women were also taking estrogen. New, lasting, or worsening mood symptoms deserve a prompt call; thoughts of self-harm need help right away.
Watch and note
Mild, brief irritability with no safety worry.
Call your prescriber promptly
Low mood, new anxiety, or a clear pattern tied to your dose that's affecting your work, sleep, or relationships.
Get help now
Thoughts of harming yourself, feeling unable to stay safe, or severe confusion. In the U.S., call or text 988.
Is spotting or bleeding normal on micronized progesterone?
Some spotting is common after starting or changing HRT, and the expected pattern depends on your regimen. Heavy bleeding, bleeding after menopause, bleeding that starts after months of calm, or anything that worries you needs a clinician’s look — not an automatic “it’s just the progesterone.”
Where you take progesterone part of each month — can cause scheduled 'withdrawal' bleeding, a bit like a light period.
Usually meant to settle into little or no bleeding over time.
The years around menopause, when hormones swing, can muddy the pattern.
A change in your estrogen can change bleeding too.
Write this down when bleeding happens:
First and last day • Light spotting or real flow • Number of pads or tampons • Any clots or pain • Where you are in your cycle.
Important safety note:if you take systemic estrogen and still have your uterus, the progesterone is protecting your uterine lining. Don’t just stop the protective part on your own because of bleeding — talk to your prescriber first.
Is micronized progesterone the “cancer hormone” I read about?
The scary “HRT causes breast cancer” headlines came from one big study — the Women’s Health Initiative (WHI) — which used estrogen plus a synthetic progestin called MPA, not micronized progesterone. In February 2026, the FDA removed the breast-cancer warning from the boxed warning on menopause hormone products — but breast cancer is still a reason not to take Prometrium.
First, the WHI mix-up
"Progestin" and "progesterone" sound alike but aren't the same. The famous WHI study used estrogen plus MPA (medroxyprogesterone acetate). In that study, combined therapy was tied to a small rise in breast cancer — about 9 extra cases per 10,000 women each year. It did not test micronized progesterone.
Second, the broader evidence
Combined estrogen-plus-progestogen therapy — of any kind — is linked to higher breast-cancer risk the longer it's used. A large analysis found women using combined products for 5 to 14 years had roughly double the risk of never-users. That's the honest backdrop.
Third, does that apply to micronized progesterone?
Not exactly. Some studies suggest micronized progesterone may carry a lower breast-cancer risk than synthetic progestins. But that evidence is limited and observational, and the FDA notes that studies haven't consistently found big differences by which progestogen is used. "May be lower than a synthetic progestin" is a fair read — not a promise of no risk.
Fourth — new in 2026: the FDA changed the labeling
On February 12, 2026, the FDA removed cardiovascular-disease, breast-cancer, and probable-dementia statements from the boxed warning for six menopause hormone products. The current Prometrium label (updated February 2026) no longer carries that boxed warning. But the current label still lists breast cancer and a history of breast cancer as a reason not to take Prometrium — and it still describes breast-cancer risk in its warnings. Removing the boxed warning did not erase that.
Do 100 mg and 200 mg micronized progesterone have different side effects?
The FDA-approved label doesn’t give a clean head-to-head comparison that would let anyone honestly say “100 mg causes X% fewer side effects than 200 mg.” Dose, schedule, your estrogen, your route, and your own body all change the picture. Any dose change belongs with your prescriber — not a chart online.
The label’s approved menopause regimen is 200 mg at bedtime for 12 days of each 28-day cycle, taken with daily conjugated estrogen — and the main side-effect table uses that 200 mg dose. There’s a separate trial at 400 mgfor missed periods, where dizziness was reported by 24% (vs. 4% on placebo) — but it’s a different dose, a different reason for taking it, and different women. It can’t be stacked into a neat “dose ladder.”
Questions worth asking your prescriber:
- What is this dose doing in my regimen?
- Is my schedule continuous or cyclic?
- Could my estrogen or another medicine be adding to this?
- Should we review the timing?
- Do my symptoms need an exam or a test?
- If we change anything, how do we keep my uterine lining protected?
Please don’t lower your dose, skip a night, or switch to using the capsule vaginally on your own to dodge side effects. Those are prescriber decisions.
Are oral, vaginal, and compounded progesterone side effects the same?
No. The FDA percentages and warnings above come from an FDA-approved oral capsule.They don’t automatically apply to vaginal use, or to custom-compounded products. Route, formula, inactive ingredients, and how much the FDA has reviewed all change what can be claimed.
FDA-approved oral progesterone (Prometrium and its generics)
This is where our data table comes from. A generic may have a different maker and different inactive ingredients, so your exact pharmacy label matters.
Vaginal use
Using this FDA-approved oral capsule vaginally is off-label in the United States — a prescriber’s judgment call outside the approved instructions. The oral trial numbers don’t transfer to vaginal use. Don’t switch routes on your own.
Compounded progesterone
Custom-compounded progesterone is not the same regulatory category as an FDA-approved product. The FDA states that compounded “bioidentical” hormones are not FDA-approved, and that it does not verify the safety, effectiveness, or quality of compounded drugs before they’re sold — and it does not have evidence they are safer, more effective, or equivalent to FDA-approved menopause hormone therapy.
Not sure which setup actually fits you? Your uterus status, estrogen route, symptoms, risk history, insurance, and state all change the right starting point.
Check which HRT care path fits your situation →Free, no email required. Provider matches are clearly labeled.
What if my Prometrium capsule contains peanut oil?
🥜 Yes — the brand-name Prometrium capsule is made with peanut oil, and the FDA label says people with a peanut allergy should not use it. If you take a generic, check the exact maker and inactive ingredients with your pharmacist rather than assuming every progesterone capsule is the same.
Brand Prometrium contains peanut oil, and peanut allergy is listed as a reason not to take it.
Generics can differ. Don't assume. Read your pharmacy label for the manufacturer, check the current package insert, and ask your pharmacist to confirm the inactive ingredients.
If you have a known peanut allergy, don't take an unverified product. Confirm it first. A severe allergic reaction — hives, swelling of the face or throat, trouble breathing — is an emergency.
Should I stop taking micronized progesterone because of side effects?
Don’t stop or change prescribed progesterone on your own — especially if it’s protecting your uterine lining while you take systemic estrogen. Stopping the progesterone part of an estrogen regimen without guidance can leave your uterine lining unprotected.
The fix might be a timing change, a dose change, or a different progestogen — and that’s a prescriber’s call. Bring these six facts to that conversation:
- Your exact product and maker
- Your dose
- Oral, vaginal, or other route
- Continuous or cyclic schedule
- Your estrogen — product, dose, and route
- When the symptom starts after your dose, how bad, and how long
What not to do on your own:double a dose, change the route, raise or lower the dose, stop the protective part of your regimen, or borrow someone else’s medicine.
Reporting a side effect: You and your clinician can report a suspected side effect to the FDA through MedWatch (the FDA’s safety-reporting program). Reporting one doesn’t prove the drug caused it — it just helps the system track patterns.
Looking to access Prometrium or a generic? See our guide to getting a Prometrium prescription online.
How we verified this page
Built with The HRT Index Verification Standard —
By The HRT Index Editorial Team. Editorial research — not reviewed by a clinician, and not a substitute for your own prescriber. We don’t invent authors, credentials, or reviewers.
What we actually verified ():
- The current FDA-approved Prometrium prescribing information — Rev. 02/2026, Reference ID 5744934 — including the Table 7 percentages, contraindications, warnings, drug-interaction notes, and peanut-oil statement
- That the current label no longer carries the boxed warning, following the FDA’s action
- The breast-cancer evidence, cross-checked against The Menopause Society, International Menopause Society, and a published meta-analysis comparing progesterone with synthetic progestins
- U.S. government patient guidance (MedlinePlus)
What we could not verify — and won’t pretend to:
- Whether your specific symptom was caused by progesterone
- Exact side-effect rates for progesterone taken alone, or for every generic maker
- Exact rates for vaginal or compounded products
- A clean 100 mg vs. 200 mg menopause comparison
Last verified: . Re-checking the FDA Prometrium label monthly; FDA labeling changes and Menopause Society positions quarterly.
Frequently asked questions
Sources
- FDA — Prometrium (progesterone, USP) prescribing information, Rev. 02/2026, Reference ID 5744934
- FDA — “FDA Approves Labeling Changes to Menopausal Hormone Therapy Products,” February 12, 2026
- FDA — Menopause / compounded “bioidentical” hormone therapy consumer guidance
- MedlinePlus — Progesterone drug information
- The Menopause Society — hormone therapy patient guidance (menopause hormone therapy and weight; individualized risk)
- International Menopause Society — statement on micronized progesterone and breast-cancer risk
- Asi N, et al. “Progesterone vs. synthetic progestins and the risk of breast cancer: a systematic review and meta-analysis.” Systematic Reviews, 2016.
- DailyMed — Prometrium listing (prescription-only; DEA schedule: none)
Update history
— Published. Verified FDA Prometrium label Rev. 02/2026, Table 7 data, contraindications, February 2026 boxed-warning removal.
The HRT Index is the independent decision resource for online menopause and HRT care. This article is educational and was not reviewed by a clinician. It is not medical advice, a diagnosis, or a substitute for your prescriber. FDA-approved and compounded options are labeled distinctly throughout; compounded products are never presented as equivalent to, safer than, or more natural than FDA-approved medication.
Still not sure which HRT path fits your body and your history?
Take our free, roughly 90-second Find My HRT Path quiz and get a personalized starting point to bring to your next consult. No email required, any provider matches are clearly labeled, and it’s built to point you to the right kind of care — including when an in-person clinician is the better first step.
Find My HRT Path → (free, ~90 seconds)