This is for you if
You use menopausal HRT, noticed spotting you weren’t expecting, and want to know whether your type of HRT and your timing change what to do — and how to walk into a visit prepared instead of panicked.
Don’t sit on this page if
You have any emergency sign above. Or you’re 12+ months past your last natural period and this is new bleeding — contact a clinician promptly rather than reading all the way through first.
The 60-second version
Find your situation, then read the section that fits.
| What’s happening | Your first move |
|---|---|
| A predictable monthly bleed on sequential (cyclical) HRT | Expected if it comes near the end of the progestogen days and isn’t heavy, long, or nonstop. Track it. Call your clinician if that changes. |
| Light spotting in the first six months of continuous combined HRT | Common while your body settles. Log it and mention it at your review. Call sooner if it gets worse. |
| New bleeding after a settled, bleed-free stretch — or 12+ months past your last period | Contact your clinician promptly for an individual check. Don’t assume it’s “just the HRT.” |
| Heavy bleeding with dizziness, weakness, or trouble breathing | ⚠ Emergency department or 911 now. See box above. |
What determines whether spotting on HRT needs checking?
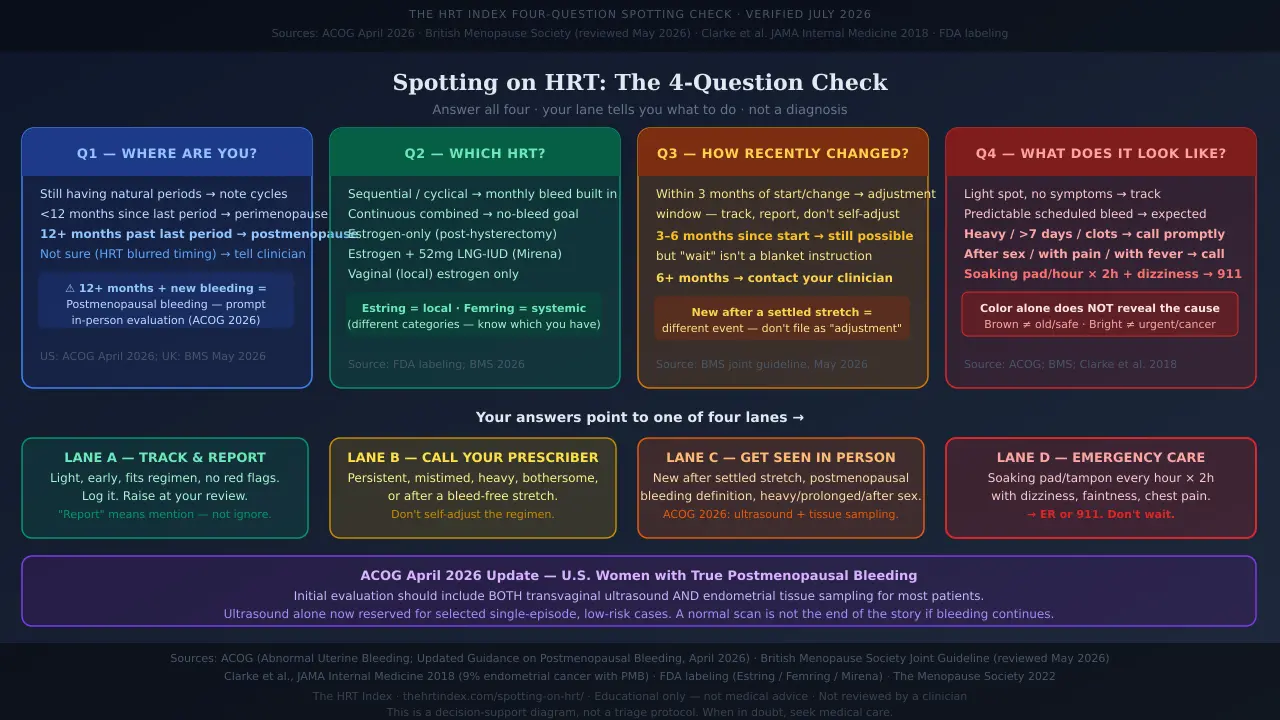
Whether spotting is “normal” depends on four things: where you are in menopause, which HRT you’re on, how recently you started or changed it, and what the bleeding looks like. Those four answers point to one of four actions.
Here’s the part most articles skip. We call this the HRT Index Four-Question Spotting Check (source review July 2026). Run through it.
Where are you in menopause?
Still having natural periods? Fewer than 12 months since your last one? More than 12 months? Or not sure, because HRT scrambled your cycle?
Which HRT are you on?
Sequential (cyclical), continuous combined, estrogen-only (after a hysterectomy), estrogen with a hormonal IUD, or vaginal estrogen only?
How recently did you start or change it?
In the last three months? The last six? Or have you been steady for longer, and this bleeding is new?
What does the bleeding look like?
Light spotting? A predictable withdrawal bleed? Period-like? Heavy or long? After sex? With pain, fever, or dizziness?
Your answers point you to a lane:
Lane A — Track and report
Fits a common early or scheduled bleed, no red flags. Keep a short log; raise it at your review.
Lane B — Call your prescriber soon
It's persistent, mistimed, bothersome, or you can't tell what's going on.
Lane C — Get seen in person
New after a settled stretch, meets the postmenopausal-bleeding definition, or has another worrying feature.
Lane D — Emergency care
Very heavy bleeding with signs of significant blood loss.
These lanes help you navigate — they aren’t a diagnosis. Only a clinician can tell you the cause.
Is spotting on HRT normal?
Spotting is a common HRT side effect, especially early on — some clinical guidance notes that unscheduled bleeding affects up to 40% of HRT users. But “normal” depends on your regimen, your menopause stage, how recently treatment changed, and whether the bleeding is light, heavy, painful, persistent, or new after a bleed-free stretch. (British Menopause Society, reviewed May 2026.)
Scheduled bleeding
Bleeding your HRT is meant to cause. On sequential HRT, a monthly bleed is built in on purpose. That’s expected.
Unscheduled bleeding
Bleeding outside that plan — any bleeding on a “no-bleed” regimen, or bleeding at the wrong time on a cyclical one. Also called breakthrough bleeding. Most common in the first six months after starting HRT and the first three months after a dose or product change — two separate clocks.
What bleeding should you expect on each type of HRT?
Sequential HRT is built to give a predictable monthly bleed. Continuous combined HRT is built to become bleed-free after a settling-in period. Estrogen-only therapy and low-dose vaginal estrogen aren’t meant to cause uterine bleeding. The delivery method doesn’t, by itself, tell you whether unexpected bleeding is harmless.
Sequential (cyclical) combined HRT
Estrogen every day, plus a progestogen for part of each cycle — typically 10–14 days, depending on the product. Often used in perimenopause or within about a year of your last period. It's designed to produce a withdrawal bleed near the end of the progestogen days, usually lasting a few days to about a week. That bleed is expected. Bleeding between those bleeds, or one that turns heavy, long, or nonstop, changes the picture.
Continuous combined HRT
Estrogen and a progestogen every single day, no breaks — usually for women past menopause who want no monthly bleed. The goal is zero bleeding, but early on, irregular light spotting is common while the lining settles, often for the first several months. That early spotting is usually the "settling-in" kind. Bleeding that shows up after six steady months, or returns after a bleed-free stretch, is a different story.
Estrogen-only HRT after a total hysterectomy
After a total hysterectomy (uterus and cervix removed), estrogen-only HRT is common, because there's no lining to protect. You shouldn't have uterine bleeding. But a subtotal or supracervical hysterectomy can leave the cervix — and sometimes a little endometrial tissue — behind. So any vaginal bleeding after a hysterectomy should be checked against your exact surgery and anatomy, not dismissed as routine.
Estrogen with a 52-mg levonorgestrel IUD (such as Mirena)
A 52-mg levonorgestrel IUD (like Mirena) can supply the progestogen that protects the lining while you take estrogen. In the United States, that use is off-label — Mirena's FDA-approved uses are contraception and heavy menstrual bleeding, not endometrial protection during menopausal estrogen therapy. Irregular spotting is very common in the first three to six months after placement, then usually fades. New heavy bleeding or bleeding after a settled stretch deserves a review.
Vaginal (local) estrogen
Low-dose local vaginal estrogen — creams, tablets or inserts, and the Estring ring — treats vaginal dryness and isn't designed to cause uterine bleeding. Minor local irritation can happen early. Important: not every vaginal ring is local. Femring delivers systemic estrogen (used for hot flashes too) and belongs in the systemic-HRT category, where a woman with a uterus needs progestogen protection. Any vaginal bleeding on local estrogen — don't wave it away. See also: our guide on vaginal estrogen. vaginal estrogen guide.
A note on compounded HRT
If your hormones come from a compounding pharmacy, know this: compounded hormone therapy is not FDA-approved, and the FDA does not have evidence that it's safer or more effective than FDA-approved products. The Menopause Society warns that compounded products carry real concerns — inconsistent dosing, possible impurities, and no standardized label of risks. Bring the exact formulation and label to any appointment, and don't self-adjust based on a bleed pattern.
| Your pattern | What it usually means | Lane | Source / where it applies |
|---|---|---|---|
| Sequential HRT, predictable bleed near end of progestogen days | A scheduled withdrawal bleed built into this regimen. Mistimed, heavy, long, or nonstop bleeding changes the answer. | A (B if mistimed/heavy/long) | NHS, UK |
| Continuous combined HRT, light spotting in the first six months | Commonly reported while the lining settles. Report at your review rather than ignore it. | A (B if it worsens or hurts) | Clinical consensus; NHS |
| Spotting within ~3 months of a dose, product, or route change | Clinician-led adjustments are expected in this window for lower-risk women. Self-adjusting is not. | A or B, by severity | British Menopause Society, UK |
| First bleeding more than 6 months after starting, or more than 3 months after a change | Outside the usual settling window. UK guidance routes this to prompt assessment, often an ultrasound. | B / C — contact your clinician promptly | British Menopause Society, UK |
| New bleeding after a settled stretch, especially 12+ months past your last period | May meet the definition of postmenopausal bleeding. U.S. guidance changed in April 2026. | C — prompt in-person evaluation | ACOG, US (April 2026) |
| Heavy or prolonged bleeding at any point | Speeds up evaluation regardless of timing. Emergency care if you have signs of major blood loss. | C, or D if emergency signs | British Menopause Society; ACOG |
| Bleeding after sex, or with pain, fever, or unusual discharge | Don't assume it's the HRT. The cervix, vagina, an infection, or another cause may need checking. | B / C | ACOG |
| You have a uterus, take estrogen, but the progestogen is missing or taken inconsistently | The lining needs adequate progestogen — this can't be safely 'balanced' by tweaking doses yourself. | B / C — clarify the regimen promptly | The Menopause Society |
| Still perimenopausal, still having natural periods | Natural cycle changes and HRT bleeding can overlap. Regimen, timing, and how different it is from your usual pattern matter more than the bleeding alone. | A / B, by severity | NHS; ACOG |
Worked out your lane, but not sure whether this is an online-care question or an in-person one?That’s what Find My HRT Path is for. It matches you to the right provider by your symptoms, route preference, insurance, and state — and it flags when online care isn’t the right place to start.
Match my situation with Find My HRT Path →What counts as heavy, prolonged, or persistent bleeding on HRT?
“Heavy” means soaking through a pad or tampon roughly every hour for several hours, or passing clots. “Prolonged” means bleeding lasting more than about seven days. “Persistent” means bleeding that keeps happening — on most days over several weeks — instead of settling. These are rules of thumb to help you describe it, not thresholds to diagnose yourself with. (ACOG; British Menopause Society.)
Flooding, clots, or soaking a pad or tampon about every hour for several hours in a row.
A bleed that runs past roughly seven days.
Light bleeding that keeps showing up on most days for weeks, rather than fading.
One caveat worth repeating: the amount of bleeding doesn’t reveal the cause — but it absolutely changes how quickly you should be seen. A small spot can still matter if it starts after a settled, bleed-free stretch. Flooding, clots, or a bleed that won’t quit needs faster attention. See the full picture at our bleeding after starting HRT guide.
How long does spotting on HRT last?
Light spotting often settles within the first six months of starting HRT, and within about three months of a dose or product change. Bleeding that begins outside those windows, or keeps going and gets worse, is worth a prompt review rather than more waiting. (British Menopause Society, reviewed May 2026; NHS.)
Peak "settling-in" time. Track the dates, how much, and any symptoms. Report it at your first review. Call sooner if it's heavy, painful, or frightening.
Still within the common window — but "wait it out" is not a blanket instruction. If it's persistent or bothering you, it deserves a conversation. Don't adjust your own progesterone to try to fix it.
Now we shift gears. Bleeding that starts (or keeps going) after six steady months moves from "probably settling" to "let's take a proper look." Contact your clinician.
This trips people up: the clock that matters is your most recent change — a new dose, a new patch, a switch from pill to gel. Six months since you first started HRT is a different marker than three months since your last change.
This is the pattern that most deserves a fresh look, and it's not the same as spotting that began the week you started. The next section explains why.
When should you get bleeding on HRT checked right away?
Get a prompt check for heavy or prolonged bleeding, bleeding with significant pain, bleeding after sex, or new bleeding after a settled stretch. Emergency care is for very heavy bleeding with dizziness, weakness, or trouble breathing. (British Menopause Society; ACOG.)
Here’s the honest catch: the amount alone can’t tell you the cause — but no website, and no telehealth screen, can tell you the cause either. Diagnosing unexpected bleeding takes an exam, and sometimes an ultrasound or a quick sample of the lining.
Emergency care — now
- Soaking a pad or tampon every hour for more than 2 hours in a row, especially with chest pain, shortness of breath, dizziness, or lightheadedness (ACOG)
- Fainting, confusion, or severe weakness
- Severe pain with bleeding, or bleeding with pain or dizziness when pregnancy is possible
Go to an emergency department or call 911. You don’t have to “earn” it by hitting every point.
Call a clinician promptly (Lane B/C)
- Heavy or prolonged bleeding, even without feeling faint
- New bleeding after a bleed-free stretch
- Bleeding after sex
- Pelvic pain, fever, or unusual discharge
- Bleeding at the wrong time on a cyclical regimen
- Spotting that keeps going past the expected settling window
- A uterus, systemic estrogen, and a progestogen that’s missing, unclear, or taken on and off
Report at your scheduled review (Lane A)
Only when it’s allof these: light, early, no red flags, fits your regimen, and not getting worse. “Report at your review” means mention it — not ignore it.
Why your risk history matters
In the current UK pathway, a BMI of 40 or higher and Lynch or Cowden syndrome are counted as major risk factors; a BMI of 30–39, diabetes, and PCOS are minor factors. Tamoxifen is a separate endometrial-risk consideration. Blood thinners can make bleeding heavier and should always be mentioned. None of this is a calculator for you to run at home — it’s a reason to give your clinician your full history. (British Menopause Society.)
What changed in U.S. postmenopausal-bleeding guidance in 2026?
In , ACOG recommended that the initial evaluation of most postmenopausal bleeding include both a transvaginal ultrasound and endometrial tissue sampling — not ultrasound alone. Ultrasound by itself is now reserved for selected patients: a single episode, a fully visualized lining no thicker than 4 mm, no strongly-associated risk factors, counseling that continued or recurrent bleeding needs immediate re-evaluation, and no significant barrier to prompt follow-up. (ACOG, April 2026.)
First, what “postmenopausal bleeding” means. It’s bleeding thought to come from the uterus 12 or more months after your last natural period. HRT can blur that line, which is why the date of your last natural periodmatters more than a simple “am I postmenopausal?”
| The older summary | What ACOG recommends as of |
|---|---|
| Ultrasound alone is the default first step | Use ultrasound and endometrial tissue sampling together for most patients with postmenopausal bleeding |
| A thin lining ends the concern in every case | Ultrasound alone is reserved for selected lower-risk, single-episode cases; it can miss an estimated 5–12% of cancers at first evaluation |
| One normal scan and you’re finished | Bleeding that continues or comes back needs immediate re-evaluation |
U.S. vs. U.K. — because they can look different
| Question | U.S. (ACOG, 2026) | U.K. (BMS, reviewed 2026) |
|---|---|---|
| Who it’s about | Postmenopausal women with any bleeding | Women with unscheduled bleeding while on HRT |
| What triggers a workup | Any postmenopausal bleeding | Bleeding outside the expected pattern; onset >6 months after starting or >3 months after a change; heavy, prolonged, or with risk factors |
| Initial assessment | Ultrasound plus tissue sampling for most | History, exam, risk-factor review; HRT may be adjusted first in lower-risk early cases |
| When is ultrasound-only okay | Only for selected single-episode, low-risk cases with a fully visualized lining ≤4 mm and prompt follow-up | A uniform lining at or below the guideline's thresholds can be reassuring; thicker or higher-risk goes to sampling |
| If bleeding recurs | Immediate re-evaluation | Re-assess and escalate |
Why the change?
Because uterine cancer keeps rising in the U.S. The American Cancer Society’s 2026 report lists uterine (endometrial) cancer among the cancers still increasing — and notes that about 68% of uterine cancers are caught early, largely because abnormal bleeding after menopause is an early warning sign. ACOG’s stated aim with the update is to reduce missed cancers and the false reassurance that ultrasound alone can give. It does notmean every spot in your first weeks of HRT needs a biopsy, and it doesn’t replace a real conversation with your clinician.
Why does HRT cause spotting?
HRT changes how the uterine lining grows and sheds, especially when treatment is new, recently changed, or out of step with your stage of menopause. But spotting can also come from polyps, fibroids, thin tissue, an infection, a missed dose, or — less often — a lining change that needs checking. The symptom alone doesn’t reveal the cause.
- Your lining adjusting. New or changed hormone levels can make the endometrium shed unevenly for a while. This is the common, early kind.
- Starting a no-bleed regimen before your body is “ready.” If you’re still cycling and go on continuous combined HRT, early bleeding can be more unpredictable.
- Missed or uneven doses. A skipped progesterone, a patch that didn’t stick, a confusing schedule. Not about blame — about telling your clinician the real story.
- Causes unrelated to your dose. Polyps and fibroids (usually benign growths), thin tissue from low estrogen, infections, and — rarely — precancer or cancer of the lining. Blood from the bladder or bowel can also be mistaken for vaginal bleeding.
| Your bleeding can hint at | Your bleeding cannot tell you |
|---|---|
| Whether the timing lines up with starting or changing therapy | Your estrogen level |
| Whether it's a scheduled or unscheduled pattern | Whether your progesterone is "too low" |
| Through amount and duration, how urgently you should be seen | Whether it is or isn't cancer |
| — | Whether the blood is from the uterus, cervix, or vagina |
Notice what’s missing from the left column: a way for youto know the cause from home. That’s not a flaw in this page — it’s the nature of bleeding.
Does spotting mean my estrogen is too high or progesterone too low?
No single bleeding pattern can prove your estrogen is too high or your progesterone too low. A dose or regimen mismatch is possible — but so are normal early adjustment, natural perimenopausal cycling, a missed dose, a polyp, or something unrelated to HRT. (The Menopause Society.)
- The same spotting can happen in several different situations.
- The color of the blood doesn’t identify the hormone.
- A single hormone blood test rarely explains the whole pattern on its own.
Please don’t cut your estrogen or double your progesterone from a search result. The one hard rule: if you have a uterus and take systemic estrogen, you need adequate progestogen to protect the lining — the FDA notes that estrogen without a progestogen raises the risk of endometrial cancer in a woman with a uterus. Quietly skipping or reducing it removes that protection. See also: HRT benefits and risks. (FDA, Menopause & Hormones.)
If you found this page while researching whether your dose is too strong, see our guide on why bleeding doesn’t prove your estrogen dose is too high.
Should you stop HRT if you start bleeding?
Don’t use an article to decide to stop, taper, or change HRT. Contact your prescriber, describe the pattern, and follow the plan you’re given. Urgent symptoms or true postmenopausal bleeding may need evaluation before your longer-term HRT plan is revisited. (The Menopause Society.)
What not to do
- Don’t double your progesterone.
- Don’t cut your estrogen.
- Don’t skip doses to “test” whether the bleeding stops.
- Don’t assume that stopping the bleeding proves HRT caused it.
What to do today
- Write down your exact regimen (medication, dose, how you take it).
- Note when you started or last changed it.
- Describe the bleeding — light, period-like, or heavy — and how long it’s lasted.
- Check the emergency signs above.
- Send your prescriber a clear message (template below).
- Follow the instructions you get back.
Copy-and-paste message for your patient portal
“I use [medication, dose, and how I take it]. I started or changed it on [date]. The bleeding began on [date] and is [spotting / period-like / heavy], lasting [how long]. I do / do not have pain, fever, dizziness, weakness, shortness of breath, or bleeding after sex. My last natural period was [date], and I do / do nothave a uterus. What do you recommend?”
What tests might a doctor do for spotting on HRT?
The evaluation may include a medication and bleeding-history review, a pelvic exam, a transvaginal ultrasound, and endometrial tissue sampling. The right order depends on your menopause stage, regimen, risk history, and current guidance. (ACOG; Contemporary OB/GYN, 2026.)
Your last natural period, your regimen, missed doses, your bleeding log, whether you still have a uterus and cervix, and whether pregnancy is possible.
Because the source might be the vagina or cervix, not the uterus.
A wand-shaped probe checks the lining's thickness and looks for growths like polyps or fibroids. Under ACOG's 2026 U.S. guidance, a fully visualized lining of 4 mm or less supports ultrasound-only evaluation only for a selected patient who meets every exception criterion — it isn't a stand-alone "all clear," and continued or recurrent bleeding needs another look regardless of the scan.
A quick office sample of the lining. As of April 2026, ACOG recommends it up front for most U.S. women with postmenopausal bleeding. It catches many endometrial cancers, but it can miss a focal spot or come back with too little tissue — so if bleeding keeps going, the workup continues even after a benign or inadequate sample.
A thin camera to look directly inside the uterus, used if bleeding continues or another test is unclear.
A pregnancy test, a blood count to check for anemia, cervical screening, or infection testing.
What if the biopsy is painful, inadequate, or normal?
Fair questions to ask your clinician before the day. Pain varies — some women feel mild cramping, others more. If the sample comes back “insufficient,” you may need another form of evaluation. And a benign result plus continued bleeding still means the workup isn’t finished. One thing to hold onto: being sent for a scan or a sample does not mean cancer has been found. The point is to find the cause instead of guessing from the bleeding.
What should you track before your appointment?
A precise record beats saying “I’ve been spotting.” Track when it started, how much, how long, any other symptoms, your medication timing, missed doses, and whether it followed sex or a patch change. (MedlinePlus.)
The bleeding
- Date and time
- Color
- How much (liners? pads?)
- Any clots
- How long it lasted
- Whether it followed sex
Your body
- Any pain, dizziness, weakness
- Fever or unusual discharge
- Feel genuinely unwell?
Your HRT
- Did you take it that day?
- Change a patch?
- Miss or delay a dose?
- Start anything new?
Your regimen, exactly
- Estradiol strength
- Patch frequency or gel pumps
- Progesterone strength and schedule
- IUD insertion date if relevant
- Photo of the packaging is perfect
Five questions worth asking at the visit
- Does my regimen fit whether I’m still cycling?
- Does this pattern need an exam, an ultrasound, or a sample?
- Is my progestogen right for my uterus status and estrogen dose?
- What change in the bleeding should send me for urgent care?
- If the first check is reassuring but bleeding continues, when do I follow up?
How does perimenopause vs. postmenopause change spotting on HRT?
In perimenopause, natural ovulation can continue while you use HRT, so bleeding may come from your cycle, the HRT, or both. Once you’re 12 months past your last natural period, new uterine bleeding is treated as postmenopausal bleeding and gets a closer look. (ACOG; NHS.)
HRT can be started before periods fully stop. Some cycle changes are expected — but report anything unusual. And HRT isn't assumed to be birth control, so if pregnancy is possible, that changes the path. See also: perimenopause symptoms checklist. See also: perimenopause symptoms checklist.
Your scheduled bleed and your natural cycle can overlap. Bleeding outside the expected pattern still deserves a review.
New bleeding is postmenopausal bleeding — and per the 2026 U.S. guidance, that's a prompt, in-person situation. Being on HRT does not remove the need to check.
Common, especially if HRT changed your bleeding. Don't force a yes/no. Tell your clinician your age, regimen, and bleeding history and let them sort it out.
Can an online HRT provider handle spotting, or do you need in-person care?
An online clinician can often review your medication timing, adherence, formulation, and whether your regimen fits your stage of menopause. But a pelvic exam, an ultrasound, a tissue sample, or evaluation of heavy, after-sex, persistent, or true postmenopausal bleeding may need an in-person gynecology visit.
Online care may be a fine starting point when
- The bleeding is light and early
- You have no warning signs
- You mainly need to sort out a regimen question or a missed dose
- Your provider can arrange local testing if needed
In-person care should come first when
- You have any emergency sign
- The bleeding meets the postmenopausal-bleeding definition
- It’s heavy, long, painful, or after sex
- An exam, scan, or sample is on the table
- Nobody’s sure where the bleeding is coming from
How did The HRT Index verify this guide?
What we checked ():
- ACOG’s update on evaluating postmenopausal bleeding, and ACOG’s emergency guidance on heavy/abnormal bleeding
- The British Menopause Society’s joint guideline on unscheduled bleeding on HRT (reviewed )
- The Menopause Society’s 2022 Hormone Therapy Position Statement and FDA menopause guidance for the compounded-hormone facts
- FDA prescribing information for Mirena, Estring, and Femring
- The Clarke et al. meta-analysis in JAMA Internal Medicine for the cancer-risk figures, and the American Cancer Society’s 2026 report for incidence
- Current NHS patient guidance on HRT side effects, plus endometrial-bleeding references from Cleveland Clinic, Yale Medicine, and StatPearls/NIH
What we did not do:
Examine you, diagnose your bleeding, or provide a medical consultation.
Last verified: using The HRT Index Verification Standard. Written by The HRT Index Editorial Team — independent editorial research, not reviewed by a clinician. Spot something out of date? Tell our editorial team.
Frequently asked questions about spotting on HRT
Same rule throughout: your regimen, timing, amount, prior stability, and other symptoms decide the next step — no general answer overrides your individual picture.
Still deciding your next step?
If you’ve read this far, you already know the two things that matter most: get red-flag bleeding checked promptly, and don’t change your HRT on a hunch. For everything in between — is this the online-care kind or the in-person kind, and which provider actually fits your situation — that’s what we built our tool for.
Still not sure which HRT program is right for you?
Take our free, private matching quiz to get matched to the right provider for your situation. Private. Educational. It matches you to a provider — it won’t diagnose you or tell you to change your medication — and it will flag when online care isn’t the right place to start.
Start Find My HRT Path →Sources
- ACOG. Updated Guidance Regarding the Role of Transvaginal Ultrasonography in Evaluating the Endometrium of Individuals With Postmenopausal Bleeding. Epub April 16, 2026.
- ACOG. Abnormal Uterine Bleeding and Heavy Menstrual Bleeding (patient FAQs).
- ACOG. Compounded Bioidentical Menopausal Hormone Therapy. Clinical Consensus, 2023.
- British Menopause Society and partner colleges. Management of Unscheduled Bleeding on Hormone Replacement Therapy (HRT): A Joint Guideline (reviewed May 2026).
- The Menopause Society (formerly NAMS). The 2022 Hormone Therapy Position Statement.
- U.S. Food and Drug Administration. Menopause & Hormones: Common Questions and menopause consumer guidance; FDA prescribing information for Mirena, Estring, and Femring.
- Clarke MA, et al. Association of Endometrial Cancer Risk With Postmenopausal Bleeding in Women: A Systematic Review and Meta-analysis. JAMA Internal Medicine, 2018.
- American Cancer Society. Cancer Statistics 2026 and Cancer Facts & Figures 2026 (uterine corpus / endometrial cancer).
- NHS. Side effects of hormone replacement therapy (HRT).
- Cleveland Clinic; Yale Medicine; StatPearls/NIH. Postmenopausal Bleeding patient references.
- Contemporary OB/GYN. Coverage of ACOG’s postmenopausal-bleeding update, 2026.
- MedlinePlus. Vaginal bleeding between periods.
— Published. Verified ACOG April 2026 postmenopausal bleeding guidance; BMS May 2026 joint guideline; Clarke et al. 2018 meta-analysis; ACS 2026 incidence figures; FDA labeling (Estring, Femring, Mirena); NHS HRT side effects guidance.
This guide is editorial research and is not medical advice. It was not reviewed by a clinician. Always talk with the professional who manages your HRT before making changes. Emergency symptoms need emergency care — don’t wait.