This guide is for you if:
- You’re in perimenopause or menopause and have been prescribed progesterone or a progestin as part of hormone therapy
- You’re figuring out whether a new symptom is normal, fixable, or a red flag
This guide is NOT for:
- Deciding a symptom’s cause from a list alone, or changing your dose on your own
- Heavy bleeding, chest pain, leg swelling, a sudden severe headache, or thoughts of harming yourself — that’s a call-now situation. Jump to urgent symptoms ↓
Start here: what to do based on what you’re feeling
Find your row. This is the fastest way to know whether you can watch and wait, should call your prescriber, or need help today.
| Your situation | What to do |
|---|---|
| Mild tiredness, dizziness, headache, breast tenderness, bloating, nausea, mood shift, discharge, or light spotting | Write down the timing and how bad it is. Contact your prescriber if it's severe, getting worse, or not settling. |
| Morning grogginess that makes driving, working, or moving around safely hard | Don't drive while impaired. Contact your prescriber to review your exact prescription and timing. |
| New or worsening depression, severe anxiety, frightening thoughts, or you can't function | Get help promptly. For immediate safety, call or text 988 (U.S.) or 911. |
| Chest pain, shortness of breath, coughing blood, face drooping, trouble speaking or seeing, arm weakness, a severe allergic reaction, confusion, or trouble walking | ⚠ Seek urgent or emergency care now. |
These groupings come from the current FDA Prometrium label and MedlinePlus drug information. Full sources are listed at the end. Want to get organized in two minutes? Jump to the 7-day symptom timeline you can copy or print.
The right online HRT provider isn’t the same for every woman — it depends on your symptoms, your age and whether you have a uterus, your medication route, your risk history, your insurance, and your state. Some situations belong with an in-person clinician first.
Find My HRT Path → (free, ~90 seconds)What are the most common progesterone side effects in menopause?
The most common side effects of oral micronized progesterone are drowsiness — taken at night because of this — plus headache, breast tenderness, dizziness, bloating, spotting, and mild stomach upset. Most are mild and often fade as your body adjusts. The catch: many overlap with menopause and estrogen, so feeling one does not prove progesterone caused it.
Three terms that get mixed up — and the mix-up leads to wrong conclusions:
The hormone your ovaries used to make, and the medicine made to match it. 'Micronized' just means it's ground into tiny particles so your gut can absorb it. Brand example: Prometrium.
A synthetic (lab-made) cousin. Different progestins have different structures and act a bit differently in the body.
The umbrella word that covers both. They are not the same, and they don't behave the same.
The current FDA patient label for Prometrium also lists a few effects people don’t always expect: hair loss, fluid retention, and vaginal yeast infection.They’re on the label — not something everyone gets, but worth knowing they’re recognized.
The FDA-label trial — with the numbers most pages hide
We pulled the current FDA-approved Prometrium label (marked Rev. 02/2026) and read the adverse-reaction table directly. It reports what happened over three years in 178 women taking cyclic Prometrium 200 mg (12 days per 28-day cycle) with conjugated estrogens, next to 174 womenon placebo. We added the “difference” column — the gap between the two groups.
Important note before you read it: these are reported event rates, not proof of cause, and not thresholds for when to worry. The treatment group took both progesterone and estrogen, so a number can reflect either drug, both together, or chance.
| Reported event | Progesterone + estrogen (n=178) | Placebo (n=174) | Difference (pct pts) |
|---|---|---|---|
| Headache | 31% | 27% | +4 |
| Breast tenderness | 27% | 6% | +21 |
| Joint pain | 20% | 29% | −9 ✓ improved |
| Depression | 19% | 12% | +7 |
| Dizziness | 15% | 9% | +6 |
| Abdominal bloating | 12% | 5% | +7 |
| Hot flashes | 11% | 35% | −24 ✓ improved |
| Urinary problems | 11% | 9% | +2 |
| Abdominal pain | 10% | 10% | 0 |
| Vaginal discharge | 10% | 3% | +7 |
| Nausea / vomiting | 8% | 7% | +1 |
| Worry | 8% | 4% | +4 |
| Chest pain | 7% | 5% | +2 |
| Diarrhea | 7% | 4% | +3 |
| Night sweats | 7% | 17% | −10 ✓ improved |
| Breast pain | 6% | 2% | +4 |
| Swelling of hands/feet | 6% | 9% | −3 |
| Vaginal dryness | 6% | 10% | −4 ✓ improved |
| Constipation | 3% | 2% | +1 |
| Breast carcinoma | 2% | <1% | — (small numbers — see note) |
| Breast excisional biopsy | 2% | <1% | — (small numbers — see note) |
| Cholecystectomy (gallbladder removal) | 2% | <1% | — (small numbers — see note) |
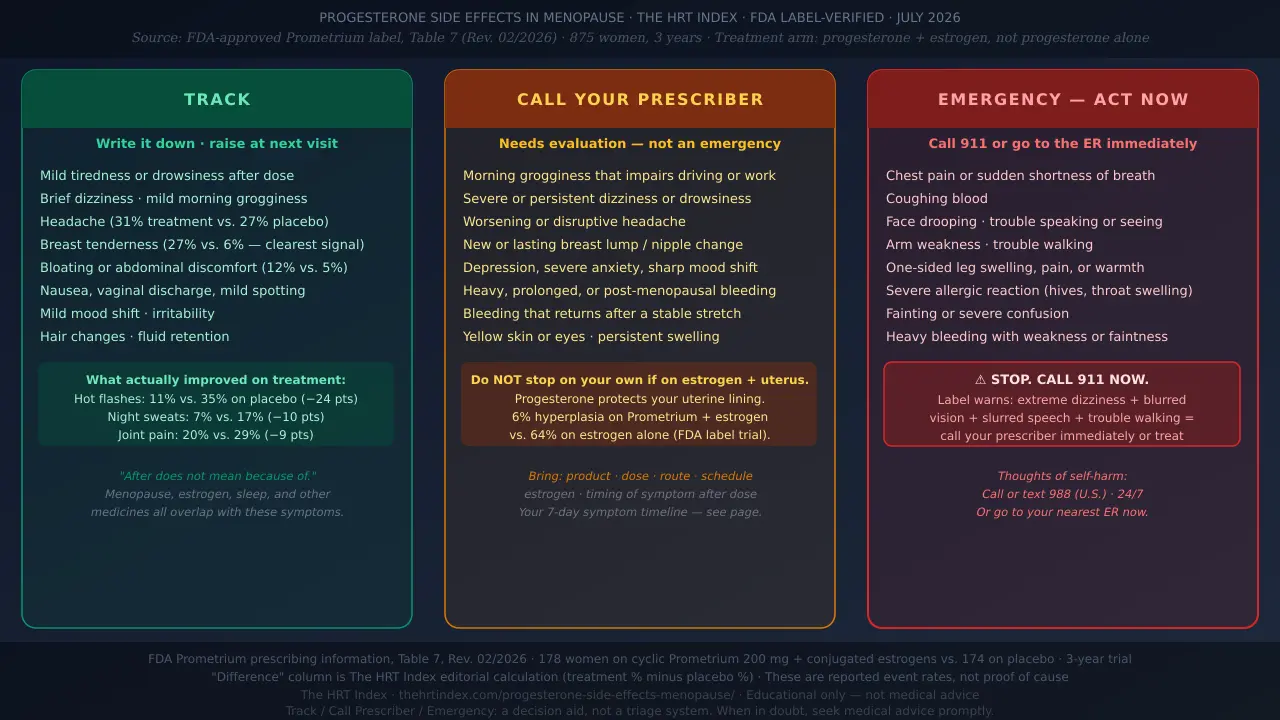
Read the bold numbers again. Hot flashes were 24 percentage points lower on treatment. Night sweats were 10 points lower. Joint pain was 9 points lower. Those aren’t progesterone side effects — they’re menopause symptoms getting better on treatment. The biggest treatment signals are breast tenderness (+21 pts), then bloating, dizziness, vaginal discharge, and depression.
The honest, uncomfortable rows:breast carcinoma at 2% vs. under 1%. In a three-year trial of only ~178 women, 2% works out to roughly three or four people — numbers that small can swing on chance, and a trial like this isn’t designed to prove cancer causation. We’re showing it because a page that hides the inconvenient numbers loses its right to be trusted on the comfortable ones.
For the full picture on side effects across the whole HRT regimen — not just the progesterone part — that page looks at the combined picture.
Which progesterone side effects are concerning, and which are urgent?
Persistent or life-disrupting symptoms deserve a call to your prescriber. A smaller set needs same-day or emergency care: chest pain, shortness of breath, coughing blood, stroke-like symptoms, a severe allergic reaction, heavy bleeding with weakness or fainting, or thoughts of self-harm.
| Level | What it looks like | What to do |
|---|---|---|
| Track | Mild, steady, not getting worse | Note the timing and severity; raise it at your next visit |
| Call your prescriber | Severe, persistent, worsening, or getting in the way of daily life | Contact the clinician who prescribed it, timeline in hand |
| Urgent / emergency | Clot, stroke, breathing, severe allergy, heavy bleeding, or immediate mental-safety signs | Seek prompt or emergency care |
The specific warning the label calls out
The FDA Prometrium label flags this: in early treatment, a small number of women have had a cluster of symptoms together — extreme dizziness or drowsiness, blurred vision, slurred speech, trouble walking, a “drunk” feeling, confusion, and shortness of breath. If that happens, contact your prescriber right away. If it comes with fainting, severe shortness of breath, or stroke-like symptoms, treat it as an emergency — not a side effect to sleep off.
A note on mental health, handled straight
The same label lists suicidal ideation among reactions reported after the drug reached the market. Two things are true at once: these reports are real, andbecause they’re collected voluntarily from an unknown number of users, the frequency and cause can’t be reliably established. So: don’t panic, but don’t brush off a serious mood change either.
If you’re in the U.S. and having thoughts of harming yourself, call or text 988 for the Suicide & Crisis Lifeline, any time. Call 911 if you or someone else is in immediate danger.
Could this be menopause, estrogen, or something else — not the progesterone?
Yes — and this is the question most pages skip. Menopause symptoms, estrogen effects, a change to your overall routine, thyroid disease, anemia, migraine, infection, lost sleep, other medicines, and plain stress can all mimic “progesterone side effects.” Timing is a useful clue. It is not proof.
Remember the table above: the placebo group had more hot flashes and night sweats than the treatment group. “It started after I began progesterone” feels like a smoking gun. Often it isn’t. After does not mean because of.
The 5-question attribution check
Run your symptom through these before you conclude anything:
- What exactly changed? The precise product and dose you started or switched to.
- Did anything else change at the same time? New estrogen, a dose change, a new medication, a rough stretch of sleep.
- How long after each dose does it hit? A repeatable “X hours after I take it” pattern supports a link — though it still doesn’t prove one.
- On a cyclic regimen, does it ease on the days you don’t take it? That on-again, off-again rhythm is a meaningful clue.
- Is there another plausible cause worth checking? Thyroid, iron, sleep, stress, another drug.
If you can’t answer #1 — “what exactly am I taking?” — that alone is worth a five-minute check, because “progesterone” could mean an FDA-approved capsule, a synthetic progestin, an IUD, or a compounded cream — and their effects and evidence differ.
Your uterus status, your estrogen, your state, your insurance, your risk history — those change the right next step, and no article can weigh them for you.
Match symptoms & history with Find My HRT Path →Free, no email required. Any provider matches are clearly labeled.
Who should not take Prometrium, and what is it FDA-approved for?
Prometrium is prescription-only, FDA-approved to prevent endometrial hyperplasia in postmenopausal women with a uterus taking conjugated-estrogen tablets, and separately to treat secondary amenorrhea. Its label lists several situations where it should not be used.
Per the current FDA label, Prometrium is contraindicated if you have any of the following:
A peanut allergy — the capsules contain peanut oil — or an allergy to any ingredient
Abnormal genital bleeding whose cause hasn't been identified
Known, suspected, or a history of breast cancer
Active deep vein thrombosis or pulmonary embolism (clot in leg or lung), or a history of either
Active arterial clot disease such as stroke or heart attack, or a history of either
Known liver problems or liver disease
The labeled menopause regimen is Prometrium 200 mg by mouth at bedtime, for 12 days of each 28-day cycle, alongside daily conjugated-estrogen tablets. Other regimens (lower continuous dose, vaginal use) can be legitimate clinician choices but are off-label. See also: full HRT contraindications guide.
Why is progesterone prescribed with estrogen in menopause?
If you have a uterus and take systemic estrogen, you generally need something to protect the lining of your uterus. Estrogen alone can make that lining overgrow (endometrial hyperplasia), which can lead to uterine cancer. Usually that protection is a progestogen. That’s why you don’t just quit it because of a side effect.
Here’s how real that protection is:
A separate endometrial-protection trial in the same FDA label followed 358 women for up to three years. Hyperplasia showed up in 6% of women on cyclic Prometrium plus conjugated estrogen, versus 64% on conjugated estrogen alone — a 58-percentage-point difference. Six percent versus sixty-four. That protection is the job your progesterone is there to do.
So when a side effect shows up, the move is almost never “quit it quietly.” It’s “review it” — the fix might be a timing change, dose change, or different progestogen, and that’s a prescriber’s call. A few situations change the picture:
You have a uterus and take systemic estrogen
You need endometrial protection — usually a progestogen. One FDA-approved option, Duavee, pairs estrogen with bazedoxifene instead of a progestogen. Dose and schedule aren't things to improvise.
You've had a hysterectomy
Many women without a uterus don't need a progestogen just for endometrial protection. But your prescription may exist for another reason — confirm with your clinician rather than stopping on the strength of a web page.
You use only low-dose vaginal estrogen
A progestogen generally isn't required with recommended low-dose vaginal estrogen — though data past a year is limited, and any unexpected bleeding still needs evaluation.
Does the type of progesterone change the side effects?
Yes — a lot. Micronized progesterone, synthetic progestins, the hormonal IUD, and compounded preparations differ in their effects, in the evidence behind them, and in their FDA status. Compare the exact product and route, not just the word “progesterone.”
| Type / form | FDA status & approved use | How taken | What to know |
|---|---|---|---|
| Oral micronized progesterone (Prometrium / generic) | FDA-approved to prevent endometrial hyperplasia in postmenopausal women with uterus on conjugated estrogens | Capsule, at bedtime | Label directs bedtime dosing due to dizziness and drowsiness. Prometrium contains peanut oil and is contraindicated with peanut allergy. Inactive ingredients vary by generic — check the specific label dispensed. |
| Vaginal progesterone | FDA-approved vaginal products are approved for fertility/luteal support — NOT menopausal endometrial protection. Using an oral capsule vaginally is off-label. | Vaginal | Don't assume vaginal progesterone is FDA-approved for protecting the uterine lining in menopause. Must be prescriber-directed. |
| Synthetic progestin — MPA (Provera) | FDA-approved | Pill | This is the progestin used in the WHI combined-therapy trial. Use the exact product label rather than assuming a universal comparison. |
| Synthetic progestin — norethindrone acetate | FDA-approved in specific products | Pill / combination | Effects and metabolic findings are product- and dose-specific; there isn't one single menopause dose. |
| Levonorgestrel IUD (e.g., Mirena) | FDA-approved for contraception and heavy menstrual bleeding. Use for endometrial protection with menopausal estrogen is off-label in the U.S. | Placed in the uterus | Releases progestin mainly locally, but systemic effects still occur (label reports headache/migraine, breast pain, depressed mood). Irregular spotting common first 3–6 months, then usually lightens. |
| Compounded progesterone (creams, troches) | NOT FDA-approved. The FDA does not verify safety, effectiveness, or quality before sale. | Varies | Absorption isn't FDA-verified. Don't assume a compounded cream provides the same uterine-lining protection as an FDA-approved regimen — supporting evidence for creams is limited and variable. |
The honest version of “is micronized safer?”
Some observational studies suggest micronized progesterone carries a lower relative breast-cancer signal — and in some analyses a lower clot signal — than certain synthetic progestins when combined with estrogen. On the other side, the FDA Prometrium label points to large studies that did not consistently find breast-cancer risk varies by which progestin is used, dose, or route. The fair takeaway: micronized progesterone is often chosen partly for a possibly gentler risk profile, but “possibly gentler” isn’t “risk-free,” and the science is still settling. That’s a conversation to have with your prescriber — not a reason to swap products based on a headline. See also: HRT benefits and risks.
Compounded, said plainly:compounded progesterone is not FDA-approved, isn’t proven equal to an FDA-approved product, and doesn’t carry the same standardized, FDA-reviewed evidence. If a cream is your progestogen and you’re on estrogen, ask specifically how your uterine lining is being protected and monitored.
How long do progesterone side effects last?
There’s no single “adjustment period” that fits every product, symptom, and woman — the current Prometrium label doesn’t set one. Many mild effects ease over the first few weeks to a few months. Early bleeding can take several months to settle. But severe, worsening, or function-limiting symptoms are not something to simply outlast.
| Timing | What to ask yourself | Reasonable next step |
|---|---|---|
| Hours after a dose | Is there a repeatable dose-to-symptom pattern? | Track it; don't drive or do risky tasks while impaired |
| First days to weeks | Is it improving, holding steady, or getting worse? | Contact your prescriber if it's severe or disruptive |
| Around 3 months | Is a mild effect still hanging around on an otherwise steady routine? | A regimen review is fair game |
| New after a long stable stretch | What else changed — a medication, sleep, health? | Don't assume it's the progesterone; get it looked at |
| Any time, with red flags | Does it match a warning sign? | Seek prompt or emergency care |
Label-backed point: oral micronized progesterone is directed to be taken at bedtime, precisely because the drowsiness and dizziness it can cause are easier to sleep through. If nobody told you that, it’s worth confirming it fits your exact prescription.
For bleeding specifically, UK menopause guidance (British Menopause Society) uses a rough rule of thumb that unscheduled bleeding often settles within about the first six months of starting HRT, or within a few months of a dose change. Use it as a general guide, not a hard rule. Don’t treat “three months” as a sentence to suffer in silence — it’s a common check-in point.
Is spotting or bleeding normal on progesterone HRT?
Spotting can happen after you start or change combined hormone therapy, and a cyclic regimen may give you a planned monthly bleed. What’s notin the “just wait” bucket: unexpected bleeding after menopause, heavier bleeding, bleeding that drags on, or bleeding that returns after things had calmed down. Report those.
| Bleeding pattern | Likely context | What to do |
|---|---|---|
| A planned bleed after the progesterone phase of a cyclic regimen | May fit the schedule | Confirm the expected pattern with your prescriber |
| Light spotting soon after starting or changing HRT | Common during adjustment | Track it; discuss at follow-up |
| Unscheduled bleeding that persists past the usual settling window on a continuous regimen | Beyond the expected adjustment period | Arrange evaluation |
| Unexpected bleeding after menopause — new after a stable stretch, heavy, or prolonged | Not explained by 'I'm on HRT' | Get it evaluated |
| Heavy bleeding with pain, weakness, or faintness | Potentially urgent | ⚠ Seek prompt care |
The one rule to remember: unexpected bleeding after menopause gets evaluated, full stop— not because it’s usually serious (it usually isn’t), but because the rare serious cause is exactly the one you don’t want to miss. An expected, scheduled bleed on a cyclic regimen is a different thing. If you’re not sure which yours is, ask. Also: a common and fixable cause of bleeding is simply missing progesterone doses — worth checking before you worry.
Can progesterone cause anxiety, depression, or low mood?
Mood changes, irritability, worry, and depression do show up in progesterone drug information — in the FDA-label trial, depression was reported in 19% on treatment versus 12% on placebo. But responses vary a lot person to person, and menopause itself drives mood symptoms. A new severe depression, suicidal thoughts, a sharp behavioral change, or an inability to function needs prompt care — not a solo experiment with your dose.
Not all “mood change” is the same. Name what you’re actually experiencing: mild irritability, more worry than usual, low mood, an abrupt and severe shift, or thoughts of self-harm. The first few are worth tracking and raising. The last two are urgent.
Timing helps: Did it start after you began or changed the medicine? Does it recur during the progesterone phase of a cyclic regimen? Did your sleep fall apart at the same time? Did estrogen change too?
Talk with a clinician sooner rather than later if you have:
- A history of severe depression, bipolar-spectrum illness, or PMDD
- Past mood changes on hormonal medicines
- Recent suicidal thoughts, or you’re badly sleep-deprived
In the U.S., call or text 988 for the Suicide & Crisis Lifeline, any time. Call 911 for an immediate emergency.
Why does progesterone make me so tired or groggy the next morning?
Because oral micronized progesterone can genuinely make you drowsy — the FDA label warns about dizziness and drowsiness and directs taking it at bedtimefor that reason. Don’t drive or do anything risky while you feel impaired, and don’t change the timing, dose, or route on your own.
To actually solve this instead of just enduring it, track the pattern for a few nights: when you took it, when you fell asleep, how many times you woke, your wake time, how alert you felt, and when the fog lifted. Note caffeine separately (it disrupts sleep in its own way), and ask a pharmacist or prescriber whether alcohol, antihistamines, sleep aids, or other medicines might be adding to the grogginess.
Next-day tiredness becomes a “call your prescriber” issuewhen it means unsafe driving, near-falls, missed work, trouble caring for people who depend on you — or if it comes with confusion, slurred speech, trouble walking, or that “drunk” feeling the label specifically warns about. That last cluster is a stop-and-call-right-away, not a sleep-it-off.
One common mistake: the bedtime instruction is specific to oral micronized progesterone. Don’t move a different progestogen — a progestin, an IUD, a cream — to bedtime on your own logic. Follow the label for the exact thing you were prescribed.
Does progesterone cause weight gain or bloating?
Bloating and fluid retention can happen — the FDA label notes progesterone may cause some fluid retention, and bloating showed up at 12% versus 5% in the trial. But a quick jump on the scale over a week or two is more likely fluid than fat. The scale alone can’t tell you which it is, and menopause itself shifts body composition. Track the trend before you blame the medicine.
Move day to day and often settle. Not the same as fat gain.
That tight, distended feeling — usually temporary.
Worth mentioning to your clinician, especially if persistent.
Over weeks, with a changing waistline — a different conversation than a two-pound blip. Bring weekly trend + timing to your prescriber.
Flag anything that comes with sudden one-sided leg swelling or shortness of breath — that’s a clot check, not a weight question.
Straight talk: progesterone isn’t a weight-loss drug, and it isn’t a reliable cause of weight gain either. Treat big promises in either direction with skepticism. For the broader picture, see: does HRT cause weight gain.
What should you do when side effects are bothering you?
Don’t guess at the cause, and don’t quietly stop a medication that may be protecting your uterine lining. The reliable path: identify your exact prescription, write down the timing and impact, check it against the warning signs, contact the person who prescribed it.
Your 7-step plan
- Read the label. Write down the exact product and active ingredient.
- Record the regimen. Dose, route, continuous or cyclic.
- Mark the change date. Include any estrogen or other medication changes.
- Track the symptom. Time after dose, how bad, how long, how much it affects your day.
- Check the warning signs. Don’t normalize an urgent symptom.
- Contact your prescriber. Bring the timeline — it makes the visit far more useful.
- Get urgent care when it’s indicated. Don’t wait for a routine appointment if you’re in a red-flag situation.
What NOT to do
- Don’t double up on a missed dose
- Don’t cut or alter a capsule unless told to
- Don’t switch routes based on an online anecdote
- Don’t treat compounded and FDA-approved products as interchangeable
- Don’t stop a uterine-protection regimen without a plan
- Don’t “push through” severe mental or neurological symptoms
Your 7-day symptom timeline (copy or print it)
This is the single most useful thing to bring to an appointment. Fill in a row each day. It won’t diagnose anything — it just turns a vague worry into a clear pattern your clinician can act on. Start tonight: jot down when you take your dose and how you feel in the morning.
| Day | Time I took it | Time I fell asleep | Next-morning alertness (1–5) | Spotting / bleeding? | Other symptoms + when they hit | Notes |
|---|---|---|---|---|---|---|
| Mon | — | — | — | — | — | — |
| Tue | — | — | — | — | — | — |
| Wed | — | — | — | — | — | — |
| Thu | — | — | — | — | — | — |
| Fri | — | — | — | — | — | — |
| Sat | — | — | — | — | — | — |
| Sun | — | — | — | — | — | — |
Bring-to-your-appointment note — fill these in too:
- Exact product and dose: ___________
- Route and schedule (continuous or cyclic): ___________
- Date started / date last changed: ___________
- Do I have a uterus? Am I also taking estrogen (and how)?: ___________
- Main symptom, and when it hits relative to my dose: ___________
- Bleeding pattern (scheduled? unscheduled? heavy?): ___________
- What I’ve already tried: ___________
Can food or other medicines change progesterone side effects?
Sometimes. In the Prometrium label’s own data, taking it with food increased how much was absorbed. And medicines that block a liver enzyme called CYP3A4 — ketoconazole is the example the label uses — may raise progesterone levels, though the label notes the real-world importance of that lab finding is uncertain.
If your clinician gave you specific instructions about food or timing, follow those over general internet advice. Before you add or stop another medication or supplement, a quick check with your pharmacist is worth it — they can spot interactions that aren’t obvious, especially anything that adds to drowsiness. Before adding a new supplement or medicine, ask.
When online menopause care isn’t the right starting point
Online care is a great fit for a lot of women — and the wrong first stop for some. It’s not right for emergencies, unexpected bleeding after menopause, severe mental-health symptoms, possible pregnancy, or symptoms that need a physical exam, imaging, or urgent testing.
Get emergency care now
Immediate self-harm danger, stroke-like symptoms, chest pain or serious trouble breathing, a severe allergic reaction, fainting or severe confusion, or heavy bleeding with weakness.
Arrange in-person care
Unexpected postmenopausal bleeding, a new breast lump or concerning breast change, persistent pelvic pain, possible pregnancy, or anything that needs a physical exam.
A complex history may need specialist care
Cancer, clots, liver disease, or neurological conditions may need specialist or in-person care. A telehealth clinician can often do an initial assessment and help figure out where you should be.
Telehealth may genuinely help
Reviewing your medication history, tracking symptoms, navigating options, and routine follow-up — when a clinician can safely manage things remotely and arrange testing or in-person care if needed.
How we researched and verified this guide
We built this from primary sources: the current FDA-approved Prometrium label (Rev. 02/2026), MedlinePlus drug information, and guidance from The Menopause Society and the British Menopause Society. Public forums were used only to understand the language women use — never to establish medical facts, rates, safety, or effectiveness.
| What we checked | How we checked it | Last verified |
|---|---|---|
| Prometrium revision date and contraindications | Read directly from the current FDA label | July 2026 |
| Trial adverse-reaction rates (Table 7) | Read directly from the FDA label; difference column is our own calculation | July 2026 |
| Endometrial-protection figures (6% vs 64%) | FDA label's separate 358-woman endometrial trial | July 2026 |
| Boxed-warning status | FDA label and FDA press announcement (2025–2026 change) | July 2026 |
| Common and serious effects | MedlinePlus and the FDA label | July 2026 |
| Compounded-product distinction | FDA compounding guidance and The Menopause Society | July 2026 |
| Bleeding-timing framework | British Menopause Society guidance (UK) | July 2026 |
| Woman-facing language | Public forum threads — language only | July 2026 |
One recent change worth knowing: in November 2025 the FDA moved to remove the prominent “boxed warnings” about heart disease, breast cancer, and dementia from menopausal hormone therapy products, with the first approved label changes — including Prometrium — taking effect in . The endometrial-cancer warning stays for systemic estrogen-alone products. The underlying risk information still lives in the label body. It’s the big warning box at the top that was removed, not the risks themselves.
Last verified: using The HRT Index Verification Standard. Research by The HRT Index Editorial Team — editorial research, not reviewed by a clinician, not medical advice.
Frequently asked questions about progesterone side effects in menopause
Still deciding what’s right for you?
Take our free Find My HRT Path quiz — about 90 seconds, and it matches your symptoms, uterus status, route preference, insurance, and state to the right path. It also flags when online care isn’t the right starting point. No pressure, and no provider pushed on you. If the quiz suggests providers, any affiliate links are labeled and rankings aren’t sold.
Get my personalized HRT path →Sources
- FDA Prometrium (progesterone, USP) Capsules prescribing information, Rev. 02/2026 — Tables 3, 5, and 7; Contraindications; Warnings; Precautions; Adverse Reactions; Patient Information.
- FDA news release: “FDA Approves Labeling Changes to Menopausal Hormone Therapy Products” — boxed-warning removal, first six products, 2026.
- Progesterone — MedlinePlus Drug Information — U.S. National Library of Medicine.
- The Menopause Society — hormone therapy, vaginal estrogen, and compounded-hormone guidance (menopause.org).
- British Menopause Society — Management of unscheduled bleeding on HRT (thebms.org.uk).
- FDA — Compounding and the FDA: Questions and Answers.
- Duavee (conjugated estrogens/bazedoxifene) prescribing information — for the estrogen-plus-bazedoxifene endometrial-protection option.
Update history
— Published. Verified FDA Prometrium label Rev. 02/2026; Table 7 adverse-reaction data; endometrial-protection trial (6% vs. 64%); contraindications; February 2026 boxed-warning removal.
This guide is educational research and is not medical advice. It was not reviewed by a clinician. Always talk with the professional who prescribed your medication before making changes. FDA-approved and compounded options are labeled distinctly throughout.