The four kinds of “no” and what each means for you. Source: Kling et al., Mayo Clinic Proceedings, 2019 (PMID 30711122) · FDA, 11/10/2025 · Verified July 2026
Four kinds of “no,” one of them means stop, and a 30-second way to check whether your doctor is reading a label the FDA has already changed.
🔎 Last verified: July 2026 · 🇺🇸 This page covers care in the United States.
The four kinds of “no” and what each means for you. Source: Kling et al., Mayo Clinic Proceedings, 2019 (PMID 30711122) · FDA, 11/10/2025 · Verified July 2026
If your doctor won’t prescribe HRT, get the exact reason before you go looking for someone who’ll say yes. The reason determines everything you do next, and there are four of them.
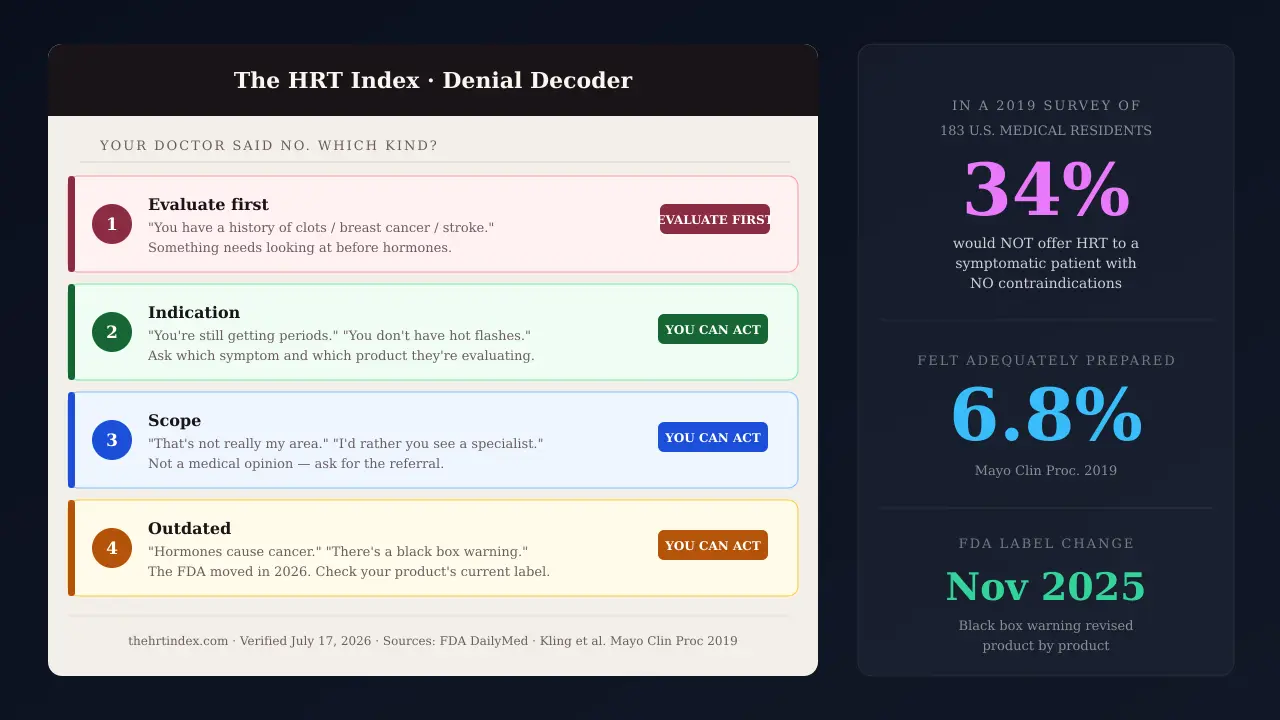
One means stop and get evaluated: unexplained bleeding, or a personal history of breast cancer, clots, stroke, heart attack, or liver disease. A provider who waves it through is a warning sign, not a win.
The other three — the wrong symptom for that product’s approved use, a clinician who doesn’t treat menopause, or a reflex left over from a 2002 study — are reasons you can act on. In a 2019 survey of U.S. medical residents, 34.4% said they would not offer hormone therapy to a symptomatic, newly menopausal woman with no contraindications at all.
| # | The “no” | What it means for you |
|---|---|---|
| 1 | Evaluate first | Something needs looking at before hormones. Not another prescriber. |
| 2 | Indication | Ask which symptom and which product they’re evaluating. |
| 3 | Scope | Not a medical opinion. Ask for the referral. |
| 4 | Outdated | Check what your product’s label actually says today. |
Not sure which one you got?
Decode my “no” → Free. No email. Takes about a minute.
| ✅ This page is for you if | ❌ This page isn’t for you if |
|---|---|
| A clinician declined to prescribe HRT and you don't know whether the reason was legitimate | You already have a prescription and it isn't working |
| You were told "too young," "come back in a year," "hormones cause cancer," or handed an antidepressant instead | You’re still deciding whether you want HRT at all → HRT benefits and risks |
| You want to know whether to re-ask, switch clinicians, or accept the answer | You’ve already shortlisted providers → Best online HRT providers |
| You're in the US | You're in the UK (the NHS pathway is different; this page won't help you) |
Scope of this page: it helps you identify the likely reason you were told no and the care setting that fits it. It does not decide whether you can take hormone therapy. Nothing here is a diagnosis. Use The HRT Index’s Find My HRT Path tool when you’re ready to match your situation to the right kind of clinician.
You have five, and they’re not equal. In rough order of what to try first:
Go back to the doctor you already have — with the specific document that answers the specific objection you got. You keep continuity, your insurance, and your record. This works more often than the internet admits.
Find a menopause-trained clinician through The Menopause Society's free directory. Costs nothing. Takes two minutes.
Buy one cash-pay second opinion and fill the prescription on your own insurance at your own pharmacy.
Start menopause-focused telehealth, which may bill your insurance for the visit.
Accept that the answer is no for systemic hormones — and get the treatment that is right for you, which may be a local product or a non-hormonal prescription with real evidence behind it.
Which of those five is yours depends entirely on why you were told no. So start there.
Most refusals come down to one of four things: something in your history that needs evaluating first, the absence of an approved indication for your specific symptom and product, a clinician who doesn’t treat menopause, or lingering caution from the 2002 Women’s Health Initiative study. In a survey of U.S. medical residents published in 2019 in Mayo Clinic Proceedings, only 6.8% felt adequately prepared to manage menopausal patients — and 34.4% said they would not offer hormone therapy to a symptomatic, newly menopausal woman with no contraindications.
Researchers surveyed 183 residents across 20 U.S. residency programs in family medicine, internal medicine, and obstetrics and gynecology. They were given a clinical vignette: a symptomatic, newly menopausal woman with no contraindications. A textbook candidate.
34.4% said they would not offer her hormone therapy.
| Finding | Number |
|---|---|
| Felt adequately prepared to manage menopausal patients | 6.8% |
| Would NOT offer HT to the symptomatic, newly menopausal vignette patient with no contraindications | 34.4% |
| Would prescribe HT until the natural age of menopause for a prematurely menopausal woman | 38.7% |
| Received NO menopause lectures during residency | 20.3% |
| Said menopause training was important or very important | 93.8% |
Source: Kling JM, et al. Mayo Clin Proc. 2019. PMID 30711122.
Read the last row again. 93.8% of them said it mattered.They knew. They weren’t taught.
You are not a difficult patient. You asked a reasonable question of someone who, statistically, may not have been taught the answer.
The Women’s Health Initiative stopped its estrogen-plus-progestin arm in 2002 and its estrogen-alone arm in 2004. The headlines were catastrophic. Prescribing collapsed. And most of the clinicians practicing today learned menopause medicine in the wreckage.
Here’s what the FDA itself said about that, in writing, on November 10, 2025: the WHI’s primary aim was to study hormone therapy’s effect on chronic disease in postmenopausal women with an average participant age of 63. Women typically get bothersome hot flashes much earlier — the average age of menopause in the U.S. is 51. In the FDA’s words, the age-related health conditions in the WHI population did not match the typically younger and healthier women who may start hormone therapy for hot flashes.
That’s not an activist reading the study generously. That’s the regulator that wrote the warning, revisiting it.
| What the FDA counted | Number |
|---|---|
| U.S. women aged 45–64 in 2020 — the ages when hot flashes are most common (U.S. Census Bureau) | ~41 million |
| Prevalence of moderate-to-severe hot flashes, women aged 45–65 (Nappi et al., 2021) | ~34% |
| U.S. women aged 46–65 who received a systemic estrogen prescription in 2020 (FDA drug utilization review) | ~2 million |
The FDA drew one conclusion, in its own words: hormone therapy may be under-utilized among women likely to benefit from it. You are not an outlier. You are the pattern.
This has a name and a shape, and it isn’t you.
Decode my “no” →You’ll know which of the four you got, what to ask next, and where to go. No email required.
The sentence your doctor used points to a likely category, but you need the documented reason to know what actually drove the decision. “You’ve had a clot” points to evaluate-first. “You’re still getting periods” points to an indication question. “That’s not really my area” is a scope answer, not a medical opinion. “Hormones cause cancer” may be out of date — though it’s worth checking your label before you assume that.
| # | The “no” | What you’d have heard | What’s behind it | Current guidance | Your next move |
|---|---|---|---|---|---|
| 1 | Evaluate first | “You have a history of clots / breast cancer / stroke.” “You’ve had bleeding we haven’t looked into.” | A condition listed in the FDA label’s Contraindications section, or something that needs a workup before hormones are on the table. | Yes. A provider who says yes without asking is a red flag, not a win. | Evaluation, not a new prescriber. See when “no” is right |
| 2 | Indication | “You’re still getting periods.” “You don’t have hot flashes.” “Come back when you’re actually in menopause.” | Each product is approved for specific symptoms. Prescribing outside that is off-label, which many clinicians do routinely and some won’t do at all. | Partly. The label limit is real. A blanket refusal to prescribe off-label is a practice choice, not a rule. | Ask which symptom and which product. How to reconsider |
| 3 | Scope | “That’s not really my area.” “I’d rather you see a specialist.” “We don’t do much of that here.” | Not a medical opinion. A capability statement. Only 6.8% of surveyed residents felt adequately prepared to manage menopausal patients. | It isn’t a clinical judgment at all, so there’s nothing to agree or disagree with. | Don’t argue. Ask for the referral. Find a clinician |
| 4 | Outdated | “Hormones cause breast cancer.” “You’re too young.” “Let’s try an antidepressant first.” “There’s a black box warning.” | The 2002 reflex, still running. But check before you assume: on some products that boxed warning language is still printed, and on others it was removed in February 2026. | The FDA formally moved — requesting removal in November 2025. Whether your label reflects it is a checkable question. | Look up your product. Bring the document. What changed in 2026 |
The part nobody tells you:any of these four can still end in a no once someone actually evaluates you. A #2 or #3 or #4 isn’t a guarantee. What it is, is a reason — and a reason is the thing you were sent home without.
Got a likely #2, #3, or #4? Each one has a different path — and a different kind of clinician at the end of it.
Find My HRT Path →Sometimes your doctor is right. The FDA label for the product in your hand lists specific conditions under Contraindications, and they’re roughly consistent across systemic estrogen products: undiagnosed abnormal genital bleeding, current or past breast cancer, estrogen-dependent tumors, active or prior DVT/PE, active or prior stroke or heart attack, hepatic impairment or disease, and known thrombophilic disorders. If that’s why you were told no, the answer is genuinely no — and the way forward is evaluation, not a different checkout page.
We earn a commission if you start care with some of the providers further down this page. Knowing that, here’s the part that costs us money to say:
If you have a real contraindication, a yes is the worst outcome available to you on this page. Worse than the no you already got. A provider that will write you an estrogen prescription without asking about clots, cancer history, liver disease, and unexplained bleeding isn’t giving you access. It’s skipping the part that protects you, and charging you for the privilege.
So this page starts by helping you tell the difference, and it will tell you to close the tab and call someone local if that’s the answer. We’d rather say it now than take your money.
Below is Section 4 of the current FDA prescribing information for estradiol gel 0.1%— one specific systemic estrogen product, revised 2/2026. This is close to what a doctor is looking at when they say “the label says I can’t.”
Estradiol gel is contraindicated in women with any of the following conditions:
- •Abnormal genital bleeding of unknown etiology
- •Current or history of breast cancer
- •Estrogen-dependent neoplasia
- •Active DVT, PE, or history of these conditions
- •Active arterial thromboembolic disease (for example, stroke or MI), or a history of these conditions
- •Known anaphylactic reaction, angioedema, or hypersensitivity to estradiol gel
- •Hepatic impairment or disease
- •Protein C, protein S, or antithrombin deficiency, or other known thrombophilic disorders
Source: DailyMed, estradiol gel 0.1%, Padagis Israel Pharmaceuticals, Set ID 3ac905b3-904c-4285-97ed-e787d006c7dd, revised 2/2026. Checked July 17, 2026. Read that as one product’s list, not as the universal rule.Contraindications live in each product’s own label.
Family history of breast cancer is not a personal history. It doesn't appear in the contraindications section above. A clinician can still reasonably decline based on an individual risk assessment — but that's a different conversation from "the label says no," and you're entitled to know which one you're having. Ask: is this a label contraindication, or your judgment about my particular risk?
Migraine isn't in Section 4 either. On the label above, migraine appears in Warnings and Precautions — a "consider whether the benefits outweigh the risks" item, not a ban. Route, aura, blood pressure, smoking, and vascular history all matter.
High BMI, hypertriglyceridemia, gallbladder disease — risk modifiers for a shared decision, not disqualifiers.
Over 60, or more than 10 years past menopause — this is about the benefit-risk profile for starting systemic therapy being less favorable in that group. That's a genuinely different statement from "not allowed," and it's an individual conversation, not a cutoff.
If that’s your situation, online care isn’t your starting point.
See what to do when systemic HRT isn’t an option →If that wasn’t the reason you were given — keep reading. What changed in 2026 is going to matter to you.
On November 10, 2025, the FDA requested labeling changes across menopausal hormone therapy products, including removal of the cardiovascular disease, breast cancer, and probable dementia statements from the boxed warning. On February 12, 2026, it approved the first batch — six products. Twenty-nine drug companies have filed proposed changes. The rollout runs product by product, so as of today the label your doctor pictures and the label on your specific product may not be the same document.
| ✅ Requested for removal | ❌ Explicitly retained |
|---|---|
| Cardiovascular disease, breast cancer, and probable dementia language out of the Boxed Warning, for all products including local vaginal | The endometrial cancer boxed warning stays — on systemic estrogen-alone products |
| The probable dementia warning out of the labeling as a whole | Cardiovascular and breast cancer information stays in the labeling — just not in the box |
| The “lowest effective dose for the shortest amount of time” recommendation out of the Boxed Warning | Approved indications are unchanged and are product-specific |
| Added for systemic products: consideration of starting hormone therapy for moderate-to-severe hot flashes in women under 60 or within 10 years of menopause onset. Added for local vaginal products: condensed safety information focused on local use. | |
Source: FDA, 11/10/2025. Checked July 17, 2026.
“The FDA said HRT is safe now” is false,and anyone telling you that is not helping you. What the FDA said is that it re-considered the benefit/risk balance, and that the risk communication didn’t match the women most likely to start these drugs. That’s a narrower sentence. It’s also a far more useful one, because it’s the one your doctor can’t argue with.
Look again at what came out of the box: the recommendation to use the lowest effective dose for the shortest amount of time. That’s the sentence behind “I’ll give you a year, then we’ll taper you off.” It’s why women get treated like they’re on a countdown. The FDA asked for it to be removed from the boxed warning in November 2025.
And Section 2.1 of the updated labels now says something new: “Consider initiating estradiol gel in women <60 years old or <10 years since menopause onset.” That last line is worth sitting with. The counter to “you’re too young” and “let’s wait a year” is now printed in the FDA-approved prescribing information — not in a podcast. In the label.
Now the part nobody has told you. The FDA’s own public list of updated products still says six. It has said six since February 12, 2026, and the page is still stamped content current as of 02/12/2026. We checked it on July 17, 2026. Five months, no movement. Meanwhile the FDA’s own press release says 29 drug companies submitted proposed labeling changes and called those six the first batch.
| Product | Labeler | Type | Boxed warning status | Revision | Source |
|---|---|---|---|---|---|
| Prometrium | — | Progestogen alone | Updated — approved by FDA 2/12/2026 | 2026 | FDA/DailyMed label |
| Divigel | Vertical Pharmaceuticals | Systemic estrogen alone | Updated — approved by FDA 2/12/2026 | 2026 | FDA/DailyMed label |
| Cenestin | — | Systemic estrogen alone | Updated — approved by FDA 2/12/2026 | 2026 | FDA/DailyMed label |
| Enjuvia | — | Systemic estrogen alone | Updated — approved by FDA 2/12/2026 | 2026 | FDA/DailyMed label |
| Estring | — | Local vaginal estrogen | Updated — approved by FDA 2/12/2026 | 2026 | FDA/DailyMed label |
| Bijuva | — | Systemic estrogen + progestogen | Updated — approved by FDA 2/12/2026 | 2026 | FDA/DailyMed label |
| Estradiol gel 0.1% (ANDA216055) | Amneal Pharmaceuticals | Systemic estrogen alone | Updated — log states removed 2/2026. Not on the FDA's published list. | 2/2026 | FDA/DailyMed label |
| Estradiol gel 0.1% (ANDA216524) | Padagis Israel Pharmaceuticals | Systemic estrogen alone | Updated — log states removed 2/2026. Not on the FDA's published list. | 2/2026 | FDA/DailyMed label |
Which means the only reliable answer to “has my product’s label changed?” is to look up your product. And there are more of them than you’d think. Estradiol gel 0.1% alone has eight separate label records on DailyMed from eight different labelers. Same drug, same strength, same route. Different documents. Which one applies to you depends on which manufacturer’s box your pharmacy handed you.
Get the exact product name and manufacturer off your box, your pharmacy label, or the product your doctor named.
Go to DailyMed — the National Library of Medicine’s official source for FDA drug labels. Free, no account.
Search the product name. If several records come up, match the manufacturer — that's the whole point.
Open the label and look at Recent Major Changes near the top. If updated, you’ll see: Boxed Warning, Cardiovascular Disorders, Breast Cancer, Probable Dementia removed 2/2026.
Look at the boxed warning itself. If it's been updated, it'll be about endometrial cancer only.
Screenshot it. Or print it.
If your product’s label still carries the old language, your doctor was reading it correctly — and that’s genuinely useful to know, because it means you’re not arguing with a person, you’re waiting on a filing. If it’s already been updated, you’re holding a current FDA document that says something different from what you were told. Either way you stop guessing. That’s not an argument. That’s a document.
What’s in the Second Conversation Kit:a symptom and bleeding timeline you fill in; your current medication list; uterus and surgery history; space for the first clinician’s documented reason; step-by-step label lookup instructions for your product; the three questions; and a records-request template.
What isn’t in it:any statement that your doctor was wrong, or any argument that you should be treated. It’s the paperwork for a real conversation — which is the thing you didn’t get to have.
Your best option is usually the doctor you already have — you keep continuity, insurance coverage, and your record. What works isn’t debating the WHI. It’s booking a dedicated appointment, answering the specific objection you got with a specific document, and asking three questions that get a documented answer.
Do not raise this at minute 11 of a physical. Say “menopause symptom management” when you book. You are asking for a conversation that needs its own appointment, and it is entirely normal to request one.
| If your doctor said… | Bring… |
|---|---|
| "Hormones cause breast cancer" / "there's a black box warning" | The FDA's November 10, 2025 request, plus your product's current label from DailyMed. If it's been updated, the box is endometrial cancer only. If it hasn't, you'll know that too. |
| "You're too young" / "come back in a year" | Section 2.1 of the updated labels: "consider initiating in women under 60 or within 10 years of menopause onset." The FDA asked for that line to be added. |
| "We taper everyone off after a year" | The FDA requested removal of "lowest effective dose for the shortest amount of time" from the boxed warning in November 2025. |
| "You're still getting periods" | Not the label — the question: "Which symptom and which product are you evaluating, and would that regimen be on-label or off-label for me?" |
| "Family history of breast cancer" | Family history isn't personal history and isn't in the contraindications section. Ask: "Is this a label contraindication, or your judgment about my individual risk?" |
| "Your hormone test came back normal" | Section 5.20: "Serum FSH and estradiol levels are not useful in the management of moderate to severe vasomotor symptoms." That's in the FDA-approved label — not an opinion. |
“Which specific contraindication applies to me?”
“Is this a clinical decision about my history, or is this outside what you prescribe?” — this is the one that separates a #1 from a #3, and almost nobody asks it. The answers are completely different and lead to completely different next steps.
“Would you note in my record that we discussed hormone therapy, that it was declined, and the reason?” That isn’t a threat and shouldn’t be delivered as one. It’s a request for a record. But it changes the room, because a reason that has to be written down has to be a reason.
When to stop trying
If you got a #3, stop. It isn’t a persuasion problem. You cannot argue someone into training they were never given, and it isn’t their fault they weren’t given it — remember the 93.8%. Ask for the referral and go.
The Menopause Society maintains a free directory of Menopause Society Certified Practitioners — clinicians who passed a menopause competency exam and recertify every three years. It’s the strongest free starting point on this page and it takes two minutes. It’s also incomplete by design, and in a lot of the country it comes back empty or with a months-long wait.
A clinician who sat and passed a menopause competency exam. The credential runs three years and is renewed by re-examination or continuing education. It’s open to all licensed healthcare professionals — so an MSCP may be a nurse practitioner or a physician assistant rather than a physician. That is not a downgrade. In this specific area it’s frequently an upgrade, because they chose to be examined on the thing you’re there for. Nobody explains that, and it matters.
Search the free MSCP directory
Search the Menopause Society directory →Zip code search, no account. This link earns us nothing. We’re telling you that because it’s the most useful link on this page and we want you to trust it precisely as much as it deserves.
Nobody publishes these. They’re the difference between the directory helping you and the directory making you feel like there’s nobody out there.
It's not a complete list. Only members and MSCPs who asked to be included appear.
It doesn't filter by accepting new patients. Many listed clinicians have 3–6 month waits.
It's geographically thin in some states. In rural areas, the closest result may be hundreds of miles away.
It doesn't distinguish between in-person only and telehealth-available clinicians.
Telehealth closes the geographic gap for a #3 or #4 scenario. Use the provider comparison below when you’re ready. Use the quiz first if you’re not sure which path is yours: Find My HRT Path →
Bring the first clinician’s documented reason, your symptom and bleeding timeline, your current medication list, your surgical history including whether you still have a uterus, and any relevant imaging or pathology. A second clinician evaluating you with your actual records is a second opinion. One evaluating you without them is just a different person guessing.
The single most valuable item on that list is the documented reason you were declined.Not your memory of the sentence — the note. You can request your records from any practice; it’s routine and you don’t have to explain why.
Bring it tothe next clinician, not around them. If the reason was a real finding, you want the next person to see it. If it was a scope answer, you want them to see that too, because it tells them there’s no clinical objection on the table.
Disclosure: The HRT Index earns a commission if you start care with some of the providers below, and those links are marked as sponsored. It doesn’t change what we verified or the order — we put each provider where the evidence puts them for this specific situation. The two most useful links on this page — The Menopause Society directory and DailyMed — earn us nothing. See our full affiliate disclosure.
If your reason was a #3 or #4 and you have a PPO, Midi Health is the strongest starting point: all 50 states, in-network with most PPO plans, live video visits with menopause-trained clinicians, and prescriptions filled at your own pharmacy. If you’re uninsured or on a high deductible, a cash-pay program like Sesame is often cheaper and lets you pick the clinician. If you’re on Medicaid, Midi cannot see you at all — not even self-pay.
| Midi Health | Sesame | Winona | |
|---|---|---|---|
| Best for | Insured (PPO), wants a menopause-trained clinician on live video, wants an FDA-approved prescription on her own plan | Uninsured / high deductible / wants to choose her own clinician | Cash-pay, no unresolved red flag, wants a specific route her doctor wouldn't write, doesn't want to wait |
| Medication | Clinicians can prescribe FDA-approved hormone options where clinically appropriate; filled at your pharmacy | Prescriptions may be sent to your preferred pharmacy | Mixed: the estradiol patch is FDA-approved. The estrogen-plus-progesterone cream is compounded and not FDA-approved. |
| Insurance | ✅ In-network with most PPO plans. Out-of-network = self-pay. | ❌ Cash-pay by design | ❌ Cash-pay |
| Medicaid | ❌ Cannot treat Medicaid or Medi-Cal patients — even as self-pay | Verify at intake | Verify at intake |
| Medicare | ❌ Not covered. Can see Medicare beneficiaries self-pay, but no claims can be submitted | Verify at intake | Verify at intake |
| Cost | $250 initial / $150 continuing (self-pay) | $59/month menopause program (provider-stated) | Estradiol patch from $149/mo; tablets $54/mo; progesterone $39/mo; compounded cream $89/mo |
| Visit format | Live video | Live video — you pick the clinician from a profile | See “what we couldn’t verify” below |
| States | All 50 | Broad — verify yours | Not all 50 — verify yours at intake |
| Testosterone | ✅ Expanded access announced Feb 2026 | Clinician-dependent | ❌ Does not prescribe |
All 50 states. In-network with most PPO plans. Live video with menopause-trained clinicians. Prescriptions go to your own pharmacy rather than a captive one. You’re not looking for hormones. You’re looking for someone who will actually do the evaluation you didn’t get— and then leave the prescription somewhere you can fill it.
⚠️ Important limitation, stated plainly:
Midi cannot treat Medicaid or Medi-Cal patients at all — not even as a self-pay patient.It isn’t covered by Medicare either; a Medicare beneficiary can pay cash but no claim can be submitted. If that’s you, Midi is not an option. And if Midi is out of network for your plan, the self-pay price is $250 for the initial visit. Check before you book, not after.
Cash-pay menopause program, provider-stated at $59/month. You read clinician profiles and pick one — which is the closest thing on the internet to the actual thing you want, which is a different person, this time chosen by me.
Prescriptions may go to your preferred pharmacy, which is the point: the visit is cash, and then you’re filling a generic on your own insurance at the counter you already use. For an uninsured woman or one with a $6,000 deductible, that combination is very often the cheapest legitimate path on this page.
Admission:no insurance billing for the visit, by design. No continuity unless you rebook the same clinician. Quality varies by clinician — which is the trade you make for getting to choose. $59/month is what its current program materials say. Confirm it at checkout before you enter a card.
Cash-pay and want to choose your own clinician? See current availability and price →Cash-pay. Text-based, so there’s no appointment slot to wait for. Winona owns its own compounding pharmacies and dispenses a mix: some FDA-approved products, and some compounded formulations.
Get the product-level distinction right:
The estradiol patch is represented by Winona as an FDA-approved product. The estrogen-plus-progesterone cream is compounded, and a compounded finished product is not FDA-approved— the FDA does not review it for safety, effectiveness, or quality before marketing.
And if your “no” was about a risk factor — a clot history, a family history, a migraine question — that conversation doesn’t belong in a text intake.Go back to the safety section. This is the wrong tool for that job and we’re not going to pretend otherwise to earn a commission.
We have an active affiliate relationship with Hers. Hers is not on this page. Hers doesn’t publish a complete menopause program price on the public page we reviewed, and it states that menopause care isn’t available in all 50 states. On a page whose entire argument is find out what it costs and what it is before you pay— we’re not sending you somewhere we can’t tell you the price. We’d make money if you clicked it. It may well be right for another situation. It isn’t right for this one.
Inner Balance isn’t here either.Its public materials describe $199/month for the first six months and $99.50/month after that, for a compounded product marketed as a whole-body treatment. A compounded finished product is not FDA-approved. Read the billing, delivery, cancellation, and guarantee terms in the actual checkout first — not the summary on the marketing page.
If a menopause-focused clinician also declines, take it seriously. Ask for the specific reason in writing, and compare it to the first one. Two declines for the same reason means there’s a real question to resolve. Two declines for different reasons means something else is going on, and that’s worth knowing too.
Same reason twice? Stop looking for a prescriber and go resolve that thing. Whatever it is, it's now the actual task.
Different reasons? Neither one is settled, and you're probably missing a record that would let someone give you a straight answer.
No reason either time? That's not a clinical finding. That's two intakes that didn't do their job.
Undiagnosed abnormal genital bleeding is contraindicated for systemic hormone therapy because it needs to be identified, not because hormones are bad. The workup is the entire point. Whatever else you do, do that.
Two declines with different reasons means something different than two declines with the same reason.
Find My HRT Path →A contraindication to systemic hormone therapy is not a contraindication to treatment. Low-dose vaginal estrogen is a local option the FDA treated separately in its 2025 request. Non-hormonal prescription options with real evidence include two FDA-approved products — fezolinetant (Veozah) and elinzanetant (Lynkuet) — plus certain SSRIs and SNRIs used off-label.
Low-dose vaginal estrogen is a local treatment with lower systemic exposure than systemic therapy, and the FDA specifically asked for its labeling to be condensed and refocused on local use — a recognition that the WHI-era warnings never fit it well.
It’s a different conversation. It is not automatic permission. If you have a history of hormone-sensitive cancer, this is a decision that may need your oncology team, and no website can make it for you. But if you were told a flat no to systemic hormones and nobody mentioned this existed, it’s worth asking about. → Vaginal estrogen
There are now two FDA-approved non-hormonal prescription drugs for moderate-to-severe hot flashes due to menopause:
Fezolinetant (Veozah) — an NK3 receptor antagonist, approved 2023
Elinzanetant (Lynkuet) — a dual NK1/NK3 receptor antagonist, approved October 2025
Both work on the brain’s temperature-regulating pathway rather than on hormones. If you have a genuine contraindication to estrogen, these were built for you, and the second one is new enough that a clinician who last read about this in 2023 may not have it on their list. Certain SSRIs and SNRIs are also used, most off-label. → Non-hormonal options
A no to systemic hormones is not a no to treatment. See the non-hormonal options →"You're too young."
Age alone isn’t a disqualifier, and the updated labels now say to consider starting in women under 60 or within 10 years of menopause. If you have primary ovarian insufficiency or early menopause, the guidance runs the other way entirely — ACOG describes hormone therapy at least until the average age of menopause, around 50–51, absent contraindications. A “you’re too young” to a woman with POI is a serious error, and it happens.
"Your family history of breast cancer."
Not a personal history, not in the contraindications section. It can still factor into an individual risk judgment. Ask which one you’re getting. → HRT benefits and risks
"You don't have hot flashes."
This is an indication problem, not a verdict on you. Products are approved for specific things — some estradiol products only for moderate-to-severe hot flashes; others for vaginal and vulvar symptoms; some for osteoporosis prevention. Brain fog, joint pain, and mood are not standalone approved indications. → Perimenopause symptoms checklist
"You're still getting periods."
Still cycling doesn’t answer whether a particular product and regimen are appropriate. The clinician needs to identify the symptom, the product’s indication, your bleeding pattern, and whether you still need contraception. Some use during perimenopause is off-label. → Perimenopause symptoms checklist
"Your migraines."
Migraine isn’t in the contraindications section; it appears under warnings about conditions that may be exacerbated. Route, aura, blood pressure, and vascular history all matter. It’s a conversation, not a door. → HRT benefits and risks
"Your clot history."
This one is in Section 4. Active DVT or PE, or a history of them, and known thrombophilic disorders. This is an evaluate-first no. → See when “no” is the right answer
Reading a provider’s own page tells you what the provider says. It doesn’t independently confirm that the claim is true in practice. We label those differently, because the difference is the whole job.
| What | Evidence level | Source | Checked | Re-check |
|---|---|---|---|---|
| FDA labeling-change request, and exactly what was removed vs retained | Primary source | FDA drug alert, 11/10/2025 | July 17, 2026 | Quarterly |
| Six products approved 2/12/2026; 29 companies submitted proposed changes | Primary source | FDA press release, 02/12/2026 | July 17, 2026 | Quarterly |
| FDA's updated-products list still shows six, still stamped 02/12/2026 | Primary source | FDA tracking page | July 17, 2026 | Monthly — this moves |
| Estradiol gel boxed-warning removal, contraindications, FSH line, under-60 initiation line | Primary source | DailyMed, Amneal and Padagis labels, both revised 2/2026 | July 17, 2026 | Monthly |
| Resident menopause-training figures | Peer-reviewed | Kling et al., Mayo Clin Proc 2019, PMID 30711122 | July 17, 2026 | Never — fixed publication |
| Midi pricing, Medicaid/Medicare limits, PPO network status | Provider-stated | Midi's own pricing and insurance page | July 17, 2026 | Monthly |
| Sesame program price and included-labs policy | Provider-stated | Sesame's own program materials | July 17, 2026 | Monthly |
| Winona product prices and FDA status | Provider-stated | Winona's own product pages | July 17, 2026 | Monthly |
| MSCP directory scope and limitations | Primary source | The Menopause Society's own directory terms | July 17, 2026 | Quarterly |
What we could not verify
Byline: Researched and written by the HRT Index Editorial Team. This page is independent editorial research. It is not medical advice and has not been reviewed by a clinician — see our medical review policy. Every medical and regulatory claim is cited to a primary source. Found an error? Tell us.
Yes. A clinician isn't required to prescribe any medication they don't believe is right for you, or that falls outside what they treat. That's not the same as being told you can't have it — it means this clinician won't write it, and you're free to ask another and to ask why.
A clinician needs prescribing authority within their professional scope and legal authorization to treat you where you're located. Within that, whether they will comes down to training and comfort, not credentials. Plenty of primary care physicians and nurse practitioners prescribe HRT routinely; plenty of gynecologists don't.
A second licensed clinician can evaluate you and reach their own conclusion. Estradiol and progesterone aren't federally scheduled controlled substances, but they're still prescription drugs, and the clinician still has to be licensed where you are and actually evaluate you. A platform that prescribes without asking about clots, cancer history, or unexplained bleeding isn't giving you access — it's skipping the evaluation.
On the current estradiol gel 0.1% label (revised 2/2026): undiagnosed abnormal genital bleeding; current or past breast cancer; estrogen-dependent tumors; active or prior DVT or PE; active or prior stroke or heart attack; hepatic impairment or disease; and known thrombophilic disorders. Other products' labels are similar but not identical — check the one you were prescribed or offered.
Family history isn't personal history and isn't listed in the contraindications above. A clinician may still decline based on an individual risk assessment. Ask which of the two you're getting — you're entitled to know.
Partly, and product by product. In November 2025 it requested removal of the cardiovascular, breast cancer, and probable dementia language from the boxed warning. The endometrial cancer boxed warning stays on systemic estrogen-alone products, and cardiovascular and breast cancer information stays in the labeling — just not in the box. Six products were approved on February 12, 2026; 29 companies have filed.
Because it might. The change rolls out product by product, so as of mid-2026 the same drug from different manufacturers can carry different labels. Look up your specific product and manufacturer on DailyMed.
No. The estradiol gel label states directly that serum FSH and estradiol levels aren't useful in managing moderate-to-severe hot flashes. In perimenopause especially, FSH swings from week to week. Menopause is diagnosed clinically, from symptoms and cycle history.
Age alone isn't a disqualifier, and the updated labels now include a line about considering initiation in women under 60 or within 10 years of menopause onset. If you have primary ovarian insufficiency or early menopause, the guidance runs the other way entirely.
Often — but understand what you're asking. These products are approved for menopausal symptoms; perimenopause isn't a standalone approved indication, so some prescribing in perimenopause is off-label. Many clinicians do it routinely. Some won't. That's a practice choice, and you're allowed to ask which one you're dealing with.
With a PPO, potentially a specialist copay, depending on your plan and deductible. Cash-pay runs from about $59/month for a menopause program up to $250 for a menopause-specialist telehealth intake. Providers state that eligible services may be paid with HSA or FSA funds; confirm with your account administrator.
Your options narrow. Midi cannot treat Medicaid or Medi-Cal patients even as self-pay. Cash-pay options exist, and many state Medicaid programs cover FDA-approved HRT at the pharmacy once you have a prescription — so the prescription and the coverage are two separate problems to solve.
A second licensed clinician can perform an independent evaluation. The first decision and your records stay clinically relevant, and you should bring them — but a decline isn't a ban, and it doesn't bind anyone else.
You came here because someone told you no and didn’t tell you why. You should leave with the why.
Our 90-second quiz matches your situation to the right kind of care — including telling you when online care isn’t the right starting point.
Take the free 90-second quiz — Find My HRT Path →