Does Medicare Part D Cover HRT for Menopause?
Yes.Medicare Part D covers FDA-approved HRT for menopause—estradiol patches, pills, gels, vaginal creams, progesterone—when your exact product is on your plan’s covered drug list. Compounded hormones are a different animal, and the answer there depends on one thing almost nobody checks: what’s actually in the jar. In 2026 your deductible is capped at $615 and your out-of-pocket at $2,100.
That’s the short answer. Here’s the part that actually matters. “Not covered” is not one thing. Sometimes it means a rule stopped the claim and your doctor can clear it in 72 hours. Sometimes it means you’re in a 90-day window that entitles you to a free month’s supply you have to know to ask for. And sometimes it means the medication isn’t a Medicare drug at all—which is the only version with no appeal.
Almost nobody hands you that distinction. You have to ask for it by name. We built this page by reading the actual federal regulations—42 CFR §423.120 and §423.578—plus the CMS rules manual, the 2026 payment memos, and each telehealth company’s own policy pages.
Editorial insurance research. Educational only—not medical advice, and not medically reviewed by a clinician. This page cannot give you an official Medicare coverage decision. Only your plan can do that.
This page is for you if:
- Your pharmacy just rejected your patch, cream, pill, gel, ring, or progesterone
- You’re turning 65 and losing the coverage that used to pay for your HRT
- Your copay jumped and you don’t know why
- You’re comparing Part D plans and want to know if your hormones will be covered
- Your doctor said “just appeal it” and you have no idea what that means
This page can’t tell you:
- Whether HRT is right for your body. That’s your clinician’s call, not ours.
- Your exact copay. We’ll explain why, and what to do instead.
- Whether to start, stop, or change a medication. Never make that decision from a website.
The short version
| Your question | The answer |
|---|---|
| Does Part D cover menopause HRT? | Yes, for FDA-approved products on your plan’s list |
| Does Part D cover compounded hormones? | It depends what’s in it. Most custom hormone creams and pellets have nothing in them Part D can pay for. Some compounds do. |
| Does Part D pay for my online consult? | No. Part D pays prescription claims only. Never visits. |
| Does turning 65 force me to stop? | No. There’s no age rule in Part D. |
| Can I fight a denial? | Usually yes—with a 72-hour clock and a statement from your prescriber |
| What’s the most I’ll pay in 2026? | $2,100 out of pocket—but only on covered drugs |
The HRT Index is the independent decision resource for online menopause and HRT care—comparing telehealth providers on clinical legitimacy, care quality, medication fit, price transparency, and access, with every claim verified and dated.
Does Medicare Part D cover HRT for menopause? Here’s the full answer.
Medicare Part D covers FDA-approved hormone therapy used for menopause when the exact product—the specific drug, strength, and form—appears on the enrollee’s plan formulary, or when the plan approves an exception. Part D pays prescription claims only. It does not pay a clinician’s visit or a lab claim; those are evaluated separately under Part B or a Medicare Advantage plan, or paid in cash.
Part D pays the prescription claim. Visits and labs are separate claims.
When you get HRT through any online menopause service, two separate money things happen:
- The visit. You talk to a clinician. Somebody pays for that.
- The drug. A prescription gets filled at a pharmacy. Somebody pays for that.
Two transactions. Two different payers. Part D only ever touches the second one.
So when you read “Midi takes insurance” or “is Winona covered?”—those sentences are about the visit. They tell you nothing about whether Medicare will pay for your estradiol.
One caveat:Under 42 CFR §423.120(c)(5), a Part D plan must reject a pharmacy claim that doesn’t carry an active, valid prescriber NPI—the ten-digit number every U.S. prescriber has. And under §423.120(c)(6), it must reject claims from prescribers on CMS’s preclusion list. So a licensed prescriber in good standing is a requirement. Beyond that, your plan cares what the drug is, not who chose it.
Why “on the list” is the whole ballgame
There is no Medicare HRT benefit. There’s no national list of covered hormones. Every Part D plan is run by a private insurance company, and every one builds its own formulary—the list of drugs it agrees to pay for.
Medicare does force plans to carry all or nearly all drugs in six specific categories: immunosuppressants, antidepressants, antipsychotics, anticonvulsants, antiretrovirals, and antineoplastics (cancer drugs). CMS calls them the six classes of clinical concern, set by statute under 42 CFR §423.120(b)(2)(v).
Read that list again. Menopause hormone therapy is not on it.
That single fact explains most of what happens at the pharmacy counter. Your plan is not required to carry your patch. It’s not required to carry any patch.
That said, under §423.120(b), a plan’s drug list has to be built by a pharmacy and therapeutics committee that includes practicing physicians and pharmacists, has to base decisions on scientific evidence, has to carry at least two drugs in each category and class, and has to be approved by CMS. So it’s a business decision inside a federal box. Knowing that changes how you fight. The question is never “why won’t Medicare cover this?” It’s “why won’t this plan cover this product, and what’s the rule that stopped it?”
The scale of the problem, in the FDA’s own numbers
The FDA published these figures in November 2025. About 41 million American women were between 45 and 64 in 2020. In that same year, about 2 million women aged 46 to 65 filled a prescription for systemic estrogen or estrogen-plus-progestogen.
The FDA’s own conclusion, in its own words: hormone therapy “may be under-utilized among women likely to benefit.” So if you feel like the system isn’t set up for you, you’re not imagining it. The agency that regulates these drugs said so in writing.
The right online HRT provider isn’t the same for every woman—it depends on your symptoms, your age, your medication route preference, your risk history, your insurance situation, and your state.
Use The HRT Index’s Find My HRT Path tool to match your situation to the right provider before your first consult.
Match my situation to the right HRT path →Free · About 90 seconds · No email required
Why was my Part D claim rejected?
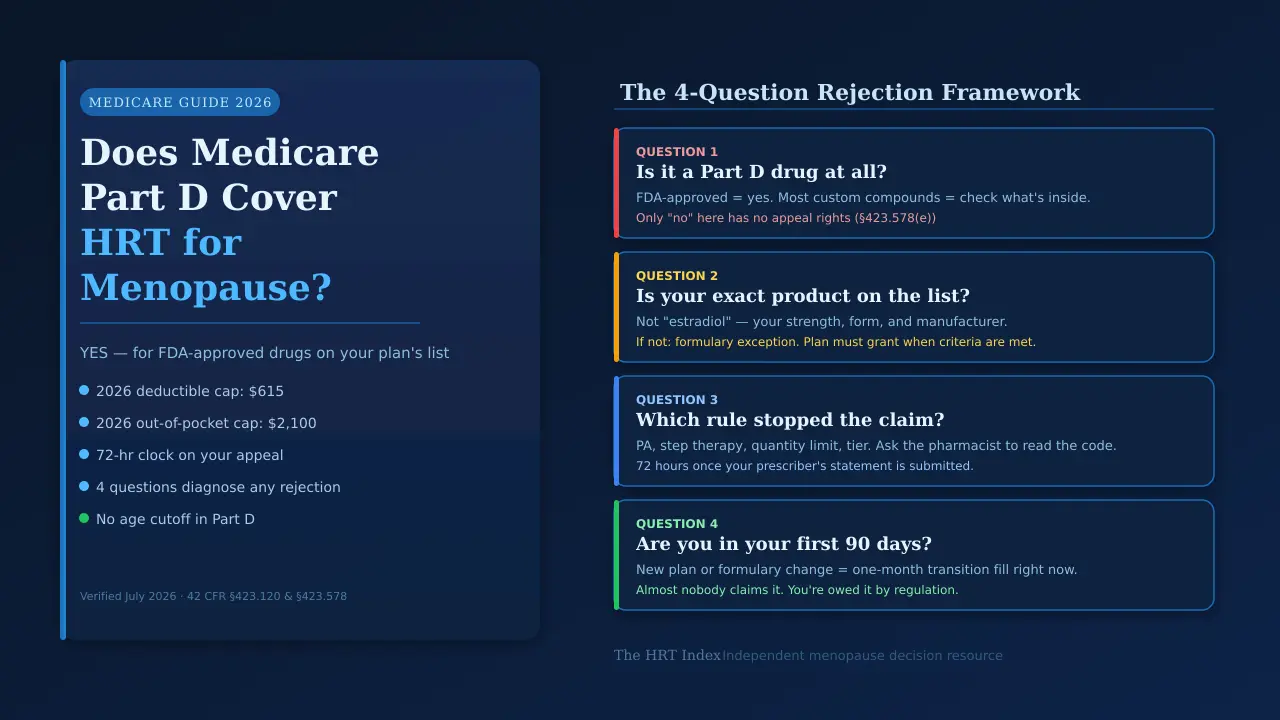
A Part D rejection has a specific cause, and the cause determines what you can do about it. Work through four questions in order: is the medication a Part D drug at all, is your exact product on your plan’s list, which rule stopped the claim, and are you inside your first 90 days on the plan. Only the first question can end with no appeal rights. The other three all have a defined next step.
This is the framework the rest of the page hangs on. We built it by reading 42 CFR §423.120 and §423.578 alongside the CMS rules manual, then mapping each legal category onto what actually gets said to women at the counter. Everyone else stops at “check your formulary.” That’s the exact moment your real problem begins.
Question 1: Is it a Part D drug at all?
This is the only gate that can lock. Under 42 CFR §423.578(e), you cannot use the exceptions process to get coverage for something that doesn’t meet the federal definition of a Part D drug. There’s no form for that. It isn’t a hard fight—it isn’t a fight. For finished, FDA-approved products—your estradiol patch, your Prometrium, your Estrace cream—this gate is not your problem. They’re Part D drugs. Move to question 2. For compounded hormones, this is the whole ballgame. We give it its own section below.
Question 2: Is your exact product on the list?
Not “estradiol.” Your product. Your strength. Your form. Your manufacturer. If it’s on the list, skip to question 3. If it’s not, you want a formulary exception—a request to cover a drug that isn’t on the list.
Question 3: Which rule stopped the claim?
This is where most rejections actually live. Ask the pharmacist to read you the reason.
| What you’re told | What it usually means | Who fixes it |
|---|---|---|
| "Not on the formulary" | Off-list product | You + prescriber → formulary exception |
| "Needs prior authorization" | Plan wants clinical documentation first | Prescriber |
| "Try something else first" | Step therapy | Prescriber → exception |
| "Quantity exceeded" | Quantity limit | Prescriber → exception |
| "Too soon to refill" | Timing edit | Pharmacy |
| "Out of network" | Pharmacy issue | You — use a network pharmacy |
| "Wrong product" | NDC or billing code mismatch | Pharmacy — often a resubmit |
| "Prescriber not valid" | Missing or inactive prescriber NPI | Pharmacy — often a resubmit |
| Tier is too expensive | Cost, not coverage | You + prescriber → tiering exception |
Some of these never reach an appeal. A refill-timing edit or a bad billing code can be fixed at the counter. Ask before you assume you’re in a fight.
Question 4: Are you in your first 90 days?
If you’re new to the plan, new to Medicare, switched plans mid-year, or your existing plan changed your drug at the start of the year—you may be owed a temporary supply right now, today, while you sort the rest out. Almost nobody claims it. Full details in the transition fill section below.
The whole framework on one screen
| Not a Part D drug | Not on the list | A rule stopped it | Tier too high | |
|---|---|---|---|---|
| What it is | Fails the federal definition | Plan's formulary choice | PA, step therapy, quantity limit | Cost-sharing placement |
| Typical cause | Most custom hormone compounds | Brand product, newer drug | Veozah, Lynkuet, brand vaginal products | Brand drugs |
| Can you appeal? | No — §423.578(e) | Yes | Yes | Sometimes — limits apply |
| Temporary supply? | No | Yes — 30 days | Yes — 30 days | No |
| Counts toward $2,100 cap? | No | Yes, once covered | Yes, once covered | Yes |
| What to file | Nothing — switch products | Formulary exception | Coverage determination / exception | Tiering exception |
Our read:the “what to file” row is The HRT Index’s editorial conclusion drawn from the verified rules above it. The rest of the table is regulation. Print this. Take it to the pharmacy. Ask which column you’re in.
Your first move takes four minutes and costs nothing
Call the number on the back of your plan card. Ask one question: “Is this exact drug, strength, and form on my formulary—and if it’s not, is it excluded from Part D entirely, or is it just not on your list?”
Those are two completely different answers. The person on the phone knows which one it is. Nobody hands you that distinction unless you ask for it by name.
Look up your plan’s 2026 formulary on Medicare Plan Finder →Free · No login · No email · Official Medicare.govWhich menopause drugs does Medicare Part D cover in 2026?
Medicare Part D can cover any FDA-approved menopause medication that a plan chooses to list, including generic estradiol tablets, patches, gels, vaginal creams, inserts, rings, micronized progesterone, and the non-hormonal drugs Veozah and Lynkuet. Coverage is decided product by product and plan by plan. No national list exists, and no page can tell you your plan’s answer.
A word about what these tables are and aren’t.The FDA status column is fact—it’s the approved label. The “what to check” column is what to ask about, not a prediction. We are not going to print a national coverage percentage we haven’t computed ourselves, and you should be suspicious of any page that does.
Systemic hormone therapy
“Systemic” means the hormone travels through your whole body. Patches, pills, gels, sprays.
| Product | What it is | FDA-approved? | What to check on your plan |
|---|---|---|---|
| Estradiol tablets (generic) | Estrogen, oral | Yes | Tier, quantity limit |
| Estradiol patch (generic) | Estrogen, through skin | Yes | Tier, quantity limit — and recheck every January. Patches are where we see the most year-to-year churn. |
| Estradiol gel (Divigel, Elestrin, EstroGel) | Estrogen, through skin | Yes | Tier, prior auth. Divigel has an updated FDA label as of Feb 2026 |
| Micronized progesterone (Prometrium, generic) | Progesterone | Yes | Tier. Updated FDA label Feb 2026 |
| Premarin | Conjugated estrogens | Yes | Brand tier, prior auth, step therapy. Keeps the estrogen-alone endometrial cancer boxed warning |
| Cenestin / Enjuvia | Synthetic conjugated estrogens | Yes | Availability, tier. Updated FDA labels Feb 2026 |
| Bijuva | Estradiol + progesterone in one capsule | Yes | Brand tier, prior auth. Updated FDA label Feb 2026 |
| Combination patches (Combipatch, Climara Pro) | Estrogen + progestin | Yes | Tier, prior auth |
| Compounded bi-est, tri-est, troches, pellets | Custom-mixed | No | Ask what's in it — see the compounding section below |
Vaginal and local estrogen
“Local” means the medicine works mostly where you put it. Creams, inserts, rings.
| Product | FDA-approved for | What to check |
|---|---|---|
| Estradiol vaginal cream (Estrace, generic) | Atrophic vaginitis due to menopause | Tier — this one swings hard |
| Premarin vaginal cream | Atrophic vaginitis, kraurosis vulvae, and moderate-to-severe dyspareunia due to menopause | Brand tier, prior auth |
| Vagifem / Yuvafem (insert) | Atrophic vaginitis due to menopause | Tier, prior auth |
| Estring (ring) | Atrophic vaginitis, urogenital symptoms | Tier. Updated FDA label Feb 2026 — the only vaginal product on the FDA's updated list so far |
| Imvexxy (insert) | Moderate-to-severe dyspareunia due to menopause | Prior auth, quantity limit |
| Intrarosa (prasterone insert) | Moderate-to-severe dyspareunia due to menopause | Prior auth, quantity limit, step therapy |
| Osphena (ospemifene, oral) | Moderate-to-severe dyspareunia and vaginal dryness due to menopause | Prior auth, quantity limit |
| Femring | Hot flashes + vulvar/vaginal atrophy | It's a ring, but it's systemic — different risk conversation |
Dyspareunia(dis-par-OO-nee-uh) is the medical word for painful sex. Atrophic vaginitis—also called vulvovaginal atrophy, or GSM, genitourinary syndrome of menopause—is thinning and drying of vaginal tissue after estrogen drops.
Non-hormonal options
| Product | FDA status | What to check |
|---|---|---|
| Veozah (fezolinetant) | FDA-approved 2023, for hot flashes | Prior auth and step therapy are common. Boxed warning for liver injury — blood tests before starting, monthly for 3 months, then at 6 and 9 months. Savings card is void on Medicare. |
| Lynkuet (elinzanetant) | FDA-approved Oct 2025 | New. Check your plan directly — formularies update through the year. Savings card void on Medicare. |
| Brisdelle (paroxetine 7.5 mg) | FDA-approved for hot flashes | Tier |
| Off-label SSRIs, SNRIs, gabapentin | Off-label for hot flashes | Whether the use counts as a "medically accepted indication" — the FDA label, or a citation in one of the drug reference compendia named in the Part D statute |
| Testosterone for women | No FDA-approved testosterone product is indicated for women in the US | Testosterone is a Schedule III controlled substance and requires a valid prescription. Part D coverage depends on the exact product and whether the use is a medically accepted indication. |
Why is my cream covered but my ring isn’t?
Medicare Part D plans do not cover the ingredient “estradiol.” They cover individual products, and a plan can list one and reject another. Coverage varies by exact drug, strength, dosage form, manufacturer and package, the code the pharmacy submits, the plan, and the pharmacy. A woman can be denied one estradiol product and approved for another on the same day.
Your plan doesn’t see “estradiol”
It sees an NDC—a National Drug Code. That’s the FDA’s identifier for a specific drug product: a ten-digit, three-part code covering the labeler, the product, and the package size.
A weekly patch and a twice-weekly patch are different products. A 0.025 mg patch and a 0.0375 mg patch are different products. Two generic patches from two different manufacturers are different products. “An estradiol patch” is not one thing to a formulary. It’s dozens.
This is why “my friend’s Medicare covers her patch” means nothing. It’s also why, when you call your plan, you read the whole label out loud—name, strength, form, quantity—instead of saying “estradiol.”
What a real prior authorization actually asks for
UnitedHealthcare’s published policy for Intrarosa approves it when all of the following are documented: a diagnosis of moderate-to-severe dyspareunia, and vulvar and vaginal atrophy due to menopause, and a history of failure, contraindication, or intolerance to two of: Imvexxy, Osphena, or Premarin vaginal cream. That’s a commercial policy, not a Medicare one—Part D plans write their own criteria. But the shape is the industry standard: diagnosis, plus the underlying condition, plus documented failure of two alternatives. Now you know what your prescriber is being asked for before the fax goes out.
What it looks like when a whole population disappears from the data
A peer-reviewed study of the Medicare Part D Spending and Prescriber Datasets tracked vaginal estrogen in the program from 2016 to 2020:
| 2016 | 2020 | Change | |
|---|---|---|---|
| Annual vaginal estrogen claims | 945,331 | 320,571 | −66% |
| Beneficiaries with a claim | 439,210 | 123,318 | −72% |
| Unique prescribers | 20,216 | 5,380 | −73% |
| Total Medicare spending | $277.9M | $106.7M | −62% |
| Mean spending per beneficiary with a claim | $688.52 | $1,027.55 | +49% |
Source: PubMed 38527966. Annual counts from claims data. Claims data can’t tell you why any individual woman stopped. Our read: something emptied out of this benefit, and nobody announced it.
Now put that next to what geriatric medicine actually recommends
The 2023 AGS Beers Criteria—the standard reference for what to avoid prescribing to older adults—says not to initiate systemic estrogen in older women, and to consider deprescribing it in women already using it.
But on vaginal estrogen, the same document says the opposite: topical vaginal estrogen remains appropriatefor symptomatic vaginal atrophy and urinary tract infection prophylaxis. The AGS’s 2025 companion paper goes further—vaginal estrogen is “the recommended first-line management strategy in most older women” for preventing recurrent UTIs. So the one hormone product that geriatric medicine actively endorses for older women is the one that quietly collapsed out of Medicare Part D.
How do I check whether my exact HRT prescription is covered?
Check the exact drug, strength, dosage form, quantity, plan, and pharmacy in Medicare Plan Finder, then confirm the result with the plan directly. The lookup shows tier and whether prior authorization, step therapy, or a quantity limit applies. Plan Finder gives an estimate; only the plan itself can give an official coverage determination.
Ten minutes. Do it in this order.
- Copy the label exactly. Not "estradiol." Get the drug name, the strength, the form, the quantity, how often you refill it, and whether it's brand or generic. The NDC is printed on the package or your pharmacy can read it to you.
- Know what coverage you actually have. Stand-alone Part D plan? Medicare Advantage with drug coverage? Medicare Advantage without drug coverage? Nothing yet? These give different answers. Your card says.
- Enter every drug you take. Not just the hormones. This is the step people skip and it's the one that costs the most. The plan with the cheapest estradiol copay is frequently a bad deal once your blood pressure medication, your statin, and your thyroid pill go in.
- Add the pharmacies you'd actually use. Preferred retail, standard retail, mail order. Same drug, same plan, different price.
- Read the restriction column. Tier, prior authorization, step therapy, quantity limit. That column is the difference between "covered" and "covered if you do paperwork first."
Then call the plan and confirm. No page online can give you your copay—not us, not anyone. It depends on your plan, your product, its tier, your pharmacy, and where you are in the year.
Look up your exact drug in Medicare Plan Finder →Official · Free · No emailWhat does HRT actually cost on Medicare Part D in 2026?
In 2026, a Medicare Part D plan may charge a deductible of up to $615, then 25% coinsurance under Medicare’s standard benefit design, until out-of-pocket spending on covered Part D drugs reaches $2,100—after which covered drugs cost the enrollee nothing for the rest of the calendar year. There is no fixed national copay for HRT.
| Parameter | 2026 |
|---|---|
| Maximum Part D deductible | $615 (some plans have none) |
| Coinsurance after the deductible, standard benefit | 25% on generics and brands |
| Annual out-of-pocket cap | $2,100 |
| After you hit the cap | $0 for covered Part D drugs, rest of the year |
| National base beneficiary premium | $38.99 |
| Late enrollment penalty | 1% × $38.99 × every full month you went without coverage |
The three things the $2,100 cap does not do
The Medicare Prescription Payment Plan
If your problem is January—the deductible and an expensive fill landing in the same month—this exists. The Medicare Prescription Payment Plan lets you spread your out-of-pocket drug costs across the calendar year instead of paying the pharmacy up front. Every plan must offer it. It’s free to join and voluntary. Medicare is blunt about what it isn’t: it “doesn’t save you money or lower your drug costs.” It’s a cash-flow tool, not a discount. But if the problem is this month, it’s a real one.
Compare 2026 plans using your full medication list →Why your $25 savings card stops working the day Medicare starts
Manufacturer copay cards for menopause medications—including the Veozah and Lynkuet savings programs—are void for people enrolled in Medicare, Medicaid, TRICARE, VA coverage, or a state pharmaceutical assistance program.
If you’re 63 with a commercial plan and your sister is 66 on Medicare, you may have access to a $25 copay and she doesn’t. Nobody explains this. It just happens.
Veozah (Astellas)
The savings card gives commercially insured patients $0 for the first month and as little as $30 per refill, up to $4,000 a year of help. Their terms state the program isn’t valid for patients whose claims are reimbursed by any state or federal government program—and then they list them: Medicaid, Medicare, Medigap, DoD, VA, TRICARE, Puerto Rico Government Insurance, or any state patient or pharmaceutical assistance program. The day your Medicare starts, you’re supposed to call and turn off your own discount.
Lynkuet (Bayer)
Same structure, blunter language. Eligible commercially insured patients may pay as little as $25 a month through Bayer’s program with BlinkRx. Their terms: patients enrolled in any type of government insurance or reimbursement program are not eligible.
These terms change. Check the program’s current page before you rely on any of this—including our summary of it.
So what replaces it?
- The $2,100 cap.This is the real answer, and it’s better than people realize. Your out-of-pocket on covered Part D drugs stops at $2,100 for the whole year, permanently, with no annual card limit and no expiration. Your 63-year-old sister with a $4,000 card limit doesn’t have that protection at all. But the cap only works on covered drugs—which is exactly why getting Veozah or Lynkuet onto your formulary through an exception is worth the fight.
- Patient assistance programs. Astellas runs one for Veozah (call 1-866-239-1637); Bayer runs one for Lynkuet. Both are income-tested and aimed primarily at uninsured patients. It costs you a phone call to find out.
- State Pharmaceutical Assistance Programs.These exist in some states, and Medicare confirms that SPAP contributions may count toward your out-of-pocket limit. Note: enrolling in one voids your manufacturer card—but you already lost that.
Extra Help—and the $1,500 sentence almost nobody says out loud
Extra Help, also called the Low-Income Subsidy, pays a qualifying Medicare beneficiary’s Part D premium and deductible and caps 2026 prescription copays at $5.10 for generics and $12.65 for brand-name drugs. Eligibility requires income at or below 150% of the federal poverty level and countable resources at or below $16,590 for a single person—or $18,090 if the person has notified Social Security that some resources are expected to be used for burial expenses.
| Extra Help category | Deductible | Generic | Brand |
|---|---|---|---|
| Full duals, institutionalized or getting home/community services | $0 | $0 | $0 |
| Full duals, income at or below 100% FPL | $0 | $1.60 | $4.90 |
| Full duals, 100–150% FPL | $0 | $5.10 | $12.65 |
| On a Medicare Savings Program (QMB, SLMB, QI) or SSI | $0 | $5.10 | $12.65 |
| Applied, income ≤150% FPL, resources under the limit | $0 | $5.10 | $12.65 |
One more thing. If you qualify for Extra Help or Medicaid but aren’t enrolled in a drug plan yet, Medicare’s LI NET programgives you temporary Part D coverage—and it covers Part D drugs with no network pharmacy restrictions. It’s a bridge most people have never heard of.
Check whether you qualify for Extra Help →Official Medicare page · We don’t earn a commission on this and never willDoes Medicare cover compounded or bioidentical HRT?
It depends on what’s in it. Under 42 CFR §423.120(d), a multi-ingredient compound can be covered under Part D only if it contains at least one ingredient that independently meets the federal definition of a Part D drug. Part D pays only for those qualifying ingredients, never for the compound as a whole. Compounds with no qualifying ingredient are outside Part D entirely, and under §423.578(e) the exceptions process cannot be used to cover them.
First, “bioidentical” means two different things
FDA-approved products that happen to be bioidentical.Estradiol patches. Estrace. Prometrium. Bijuva. These contain hormones structurally identical to what your ovaries made, and they’re FDA-approved finished drugs. They go through the normal formulary lookup. Part D covers them every day.
Custom-compounded “bioidentical” hormones.Mixed to order by a compounding pharmacy. The compound itself is not FDA-approved. If a company tells you their bioidentical hormones aren’t covered “because insurance doesn’t like bioidenticals”—that’s not it. FDA-approved bioidentical estradiol is covered by Medicare constantly. The issue is the compounding, not the molecule.
The actual test, in one question
That’s the whole test. Bulk active pharmaceutical ingredient—raw hormone powder—does not satisfy the Part D drug definition. Most custom bi-est and tri-est creams, troches, and compounded pellets are made from bulk powder. If that’s yours, there is no qualifying ingredient, and there’s nothing for Part D to pay. But you should ask rather than assume.
CMS Manual, Chapter 6, §10.4: “Compounded prescription drug products can contain (1) all Part D drug product components; (2) some Part D drug product components; or (3) no Part D drug product components. Only costs associated with those components that satisfy the definition of a Part D drug are allowable costs under Part D because the compounded products as a whole do not satisfy the definition of a Part D drug.”
About pellets
Compounded hormone pellets, including the BioTE-style kind, are compounded products and are not FDA-approved finished drugs. Whether Part D pays anything toward one can’t be decided from the brand name. It depends on the exact product, its ingredients, how it’s administered, whether it’s billed under Part B or Part D, and your plan’s determination. Ask your plan for a determination in writing.
If your compound has no Part D-qualifying ingredient, it’s cash, with no cap credit and no appeal. If that’s sustainable for you, fine. If it isn’t, the conversation to have with your prescriber is whether an FDA-approved product would be appropriate for your situation.
The pharmacy said no. Here’s exactly what to do.
When a Part D plan denies a menopause prescription, the enrollee or prescriber can request a coverage determination or exception. The plan must decide within 72 hours of receiving the prescriber’s supporting statement, or 24 hours if expedited. If denied, a Level 1 appeal must be filed within 65 days of the denial notice.
Step 1
Don't accept "insurance won't cover it"
That sentence is not information. Go back to the four questions above and get the actual rejection reason.
Step 2
Call the plan. Ask these five questions.
- Is this exact drug, strength, and dosage form on my formulary?
- What tier is it on?
- Does it need prior authorization, step therapy, or a quantity limit exception?
- Is there a covered alternative in the same form? (Not "a different pill." The same form.)
- What exactly does my prescriber need to send you, and where?
Question 5 ends the phone call productively. Get the form name and the fax number.
Step 3
Get the coverage determination filed
Under §423.578(b)(5), the prescriber's supporting statement can be oral or written. Your doctor can start this with a phone call. The statement must say the covered Part D drugs on any tier would not be as effective for you, would cause you adverse effects, or both — or that the formulary alternative has been ineffective or is likely to be ineffective. The plan must grant the exception when it determines the drug is medically necessary. But §423.578(f) is explicit: the statement is not a magic word. The plan makes the determination.
Step 4
If they say no, appeal within 65 days
Five levels. Most HRT cases end at level one or two.
The appeal clocks
| Request | Standard | Expedited |
|---|---|---|
| Coverage determination / exception | 72 hours | 24 hours |
| Level 1 appeal (redetermination) | 7 days | 72 hours |
| Payment reimbursement appeal | 14 days | — |
Appeal levels
| Level | Who decides | Deadline to file | Decision due |
|---|---|---|---|
| 1 — Redetermination | Your plan | 65 days from denial notice | 7 days / 72 hours fast |
| 2 — Reconsideration | Independent Review Entity | 60 days | 7 days / 72 hours fast |
| 3 — Hearing | Administrative Law Judge | 60 days | varies |
| 4 — Review | Medicare Appeals Council | 60 days | varies |
| 5 — Federal court | Judge | 60 days | varies |
For 2026: $200 to reach an ALJ hearing, $1,960 to reach federal court (Federal Register, December 4, 2025). Related denials can sometimes be combined.
Three rules that decide HRT appeals—and almost nobody publishes them
Build your exception packet before you call
Win it once, and you’re done for the plan year. Once a non-formulary exception is approved, under §423.578(c)(4) the plan may not make you request approval again for refills. But check your Annual Notice of Change in September—the plan may choose to continue coverage into the next year. May. Not must.
Build my HRT exception checklist →A note on privacy: don’t send your plan more health information than they asked for. The supporting statement is a narrow document. Keep it narrow.
Does Medicare make you stop HRT at 65?
No. Medicare has no age cutoff for hormone therapy in Part D.
| Insurance question | Medical question |
|---|---|
| Is my product on the formulary? | Is this treatment right for my body? |
| What tier, what restrictions? | What's the benefit, the risk, the dose, the route? |
| Can I file an exception? | Should I continue, adjust, or stop? |
| Answered by: your plan | Answered by: your clinician |
What the guidance actually says—all of it
The honest synthesis:
- Starting systemic HRT after 65—the guidance leans against it. The FDA’s new labeling highlights the under-60 window. Beers says don’t initiate. That’s not a prohibition, and it’s not a coverage rule. It’s a real conversation to have with a clinician who knows this literature.
- Continuing systemic HRT past 65—no automatic stop rule. The Menopause Society is clear. Beers says “consider deprescribing,” which is a conversation, not a mandate.
- Vaginal estrogen at any age—everyone agrees. Beers explicitly endorses it. It’s first-line for recurrent UTIs in older women.
The FDA changed the labels. Here’s what’s actually happened since.
On November 10, 2025, the FDA asked the makers of menopausal hormone therapies to change their labels. What it asked for:
- Cardiovascular disease
- Breast cancer
- Probable dementia
- The “lowest effective dose for the shortest amount of time” recommendation
- Kept: endometrial cancer boxed warning on estrogen-alone
- Added: under-60 / within-10-years initiation note
- Added: WHI data for women aged 50–59
On February 12, 2026, the FDA approved the first batch of updated labels: six products—Prometrium, Divigel, Cenestin, Enjuvia, Estring, Bijuva.
We checked the FDA’s list on July 16, 2026. It still says six, and the page is still marked “content current as of 02/12/2026.”Not generic estradiol tablets. Not the patch you’re wearing. Not Vagifem. Not Estrace cream. Not Premarin. The paperwork hasn’t caught up. We check this list monthly and log the date.
Can Midi, Winona, Hers, or Sesame get you HRT that Medicare Part D covers?
No menopause telehealth service we have verified bills Medicare for the visit. A Part D plan can still pay for the medication if a licensed clinician sends an FDA-approved prescription to the enrollee’s own network pharmacy and the product is covered. If a service bundles medication into a cash monthly fee and ships it from its own pharmacy, there is no Part D claim, and the spending does not count toward the annual out-of-pocket cap.
Verified July 2026 against each company’s own site. We recheck top providers monthly. Verify anything here on the company’s own page before you pay—including what we’ve written.
| Provider | Bills Medicare for the visit? | Medication model | Part D compatible? |
|---|---|---|---|
| Midi Health | No | FDA-approved (patches, pills, rings, creams, gels) | Unresolved — see below |
| Sesame | No | Prescription sent to your own local pharmacy | Structurally yes. Cash visit → your pharmacy → Part D decides the drug |
| Winona | No | Offers both compounded products and an FDA-approved estradiol patch; ships from its own pharmacy | Depends on the exact product — see below |
| Hers | No | Cash subscription | Cash |
The correction that earns us this page: the Midi situation
Several review sites currently say Midi Health accepts “some Medicare Advantage plans.” Midi says otherwise, on its own website: “Midi is not covered by Medicare or any Medicare-related insurance plan.” The full statement continues: Midi can accept Medicare beneficiaries as self-pay patients, but those beneficiaries cannot submit any claims related to their Midi visits, medications, or associated services. We marked Midi “unresolved” on the drug question because Midi’s language is broad. If you’re on Medicare and considering Midi, ask them in writing whether you may run a prescription from a Midi clinician through your own Part D plan at your own pharmacy. Then hold onto the answer. And: Midi states it cannot treat Medicaid or Medi-Cal patients at all—even as self-pay patients.
The Sesame situation—and the honest part
Sesame doesn’t bill insurance at all. You see the visit price before you book—no surprise bill, no “this is not a bill”—and the prescription goes to your own pharmacy on your own Part D plan. That’s the two-transaction model, in the vendor’s own words.
What we verified about Sesame in July 2026:it’s a marketplace of individual clinicians available in all 50 states. Telehealth visits start in the mid-$30s, and the live price is shown before you book. Prescriptions go to you or your local pharmacy.
Who Sesame is for: you don’t have a prescriber for this, or you want a second opinion, or your doctor doesn’t treat menopause and you want an FDA-approved prescription routed to your own pharmacy at a price you can see before you book. Who it’s not for:if your own doctor won’t write a supporting statement for your appeal, do not go shopping for a signature. Ask why first. A second opinion is an independent clinical judgment—it might agree with your first one.
Cash price shown before you book · All 50 states · Prescription goes to your own pharmacy
The visit is cash either way—but the drug is a separate transaction, and that’s the one your Part D plan can pay for.
Check Sesame visit prices in your state →The HRT Index earns a commission if you book through this link, at no additional cost to you. It doesn’t influence what we published above—we spent this entire section explaining why our highest-paying partner is the wrong answer for Medicare beneficiaries who want Medicare to pay for the visit.
Part B, Medicare Advantage, and Medigap: what each part actually pays for
Medicare Part B covers clinician visits and lab work under its normal rules but generally does not pay for self-administered outpatient prescriptions like patches, pills, creams, or rings—those fall under Part D. Medigap policies sold after January 1, 2006 do not include prescription drug coverage.
| What you’re paying for | Part A | Part B | Part D / MA-PD | Medigap |
|---|---|---|---|---|
| In-person gynecologist visit | No | Maybe — if covered, medically necessary, clinician accepts Medicare | No | Helps with Part B cost sharing |
| Online menopause consult (cash service) | No | No — these services don't bill it | No | No |
| Hormone blood work your doctor orders | No | Maybe — depends on the test, diagnosis, lab, and frequency | No | Helps with cost sharing |
| Estradiol patch from your pharmacy | No | No | Yes, if on formulary | No |
| Vaginal cream from your pharmacy | No | No | Yes, if on formulary | No |
| Compounded cream | No | No | Only qualifying ingredients, if any | No |
| Veozah / Lynkuet | No | No | Yes, if on formulary | No |
| Drugs during a covered inpatient stay | Generally included | No | No | Helps with Part A cost sharing |
Medicare Advantage isn’t a shortcut.A Medicare Advantage plan with drug coverage uses a Part D formulary. Same rulebook: tiers, prior authorization, step therapy, exclusions, exceptions. The plan bundles your medical and drug benefits onto one card. It does not make your hormones more covered. And one trap: not every Medicare Advantage plan includes drug coverage. If yours doesn’t, you have the same problem as someone with no Part D at all.
Medigap:policies sold after January 1, 2006 don’t include prescription drug coverage at all. Some older policies retain legacy drug coverage; if you’ve had yours since before 2006, it’s worth checking. For everyone else: Medigap is not a substitute for Part D.
Your patch got dropped in January. Now what?
Medicare Part D plans must provide a one-time transition supply of at least an approved month’s supply for a drug an enrollee was already taking that is non-formulary or newly restricted, available during the first 90 days of coverage under a new plan or new plan year. The plan must send written notice within three business days of the fill. Drugs that aren’t Part D drugs don’t qualify.
The transition fill
Under 42 CFR §423.120(b)(3), your plan must give you a one-time temporary supply of at least an approved month’s supply of a drug you were already on, during your first 90 days. It applies to new enrollees, people newly eligible for Medicare, people who switch plans mid-year, and current enrollees whose plan changed their formulary.
And here’s the part that catches people: a drug that’s on the formulary but suddenly requires prior authorization or step therapy is treated as non-formulary for transition purposes. So if your patch is technically listed but now needs paperwork, you still get the fill. Your plan must mail you written notice within three business days of that fill.
Your drug got changed mid-year? You may be protected.
Should you switch plans?
Only during an enrollment period you qualify for. And only after doing this properly: enter every drug you take (not just the hormones), check next year’s formulary even when this year is fine (your Annual Notice of Change arrives by September 30), and also compare premium, deductible, whether your pharmacy is preferred, mail-order requirements, and how heavy-handed the plan is with prior authorization.
Compare Part D plans with your complete drug list →Official Medicare tool · Free · No agent · No phone number · No sales callWhat we actually verified
This page was produced under The HRT Index Verification Standard: we read every published price, separate FDA-approved from compounded, verify state availability and insurance, and re-check on a fixed schedule.
What we opened ourselves, in July 2026:
- 42 CFR §423.120—compound rules (d), transition fills (b)(3), formulary standards (b)(1)–(2), prescriber NPI and preclusion (c)(5)–(6), formulary change limits (e), notice requirements (f), pharmacy cash-price protection (a)(8)(iii)
- 42 CFR §423.578—the exceptions process: “must grant” standard (b), the limit that a supporting statement isn’t automatic (f), bar on exceptions for non-Part D drugs (e), exception spending counting toward the cap (b)(3), tiering exception limits (a)(6), auto-forward on a missed deadline (c)(2), refill continuity (c)(4)
- CMS Medicare Prescription Drug Benefit Manual, Chapter 6—compounding (§10.4), medically accepted indication (§10.6), exclusions list (§20.1), transition rules (§30.4)
- Medicare.gov Part D costs page—$615 deductible, 25% standard coinsurance, $2,100 cap, $38.99 base premium
- CMS memo dated October 31, 2025—2026 Extra Help resource limits and copays, including the burial set-aside
- Federal Register, December 4, 2025—2026 amounts in controversy: $200 and $1,960
- FDA’s list of menopausal hormone therapies with updated prescribing information—checked July 16, 2026, still showing six products, still dated 02/12/2026
- FDA’s November 10, 2025 labeling request—what was removed, kept, and added
- The Menopause Society 2022 position statement and the 2023 AGS Beers Criteria
- A published prior authorization policy for Intrarosa—for what PA criteria actually require
- Midi Health, Sesame, and Winona’s own policy pages—for the Medicare statements quoted above
- Astellas’ and Bayer’s savings program terms—for the Medicare exclusions
- Peer-reviewed literature on vaginal estrogen use in Part D (PubMed 38527966)
What we did not verify, and won’t pretend to:your plan’s answer, your copay, whether HRT is right for you, national formulary percentages, every price on this page tomorrow.
Corrections made to this page.An earlier version stated that compounded hormones were never covered by Part D, never appealable, and never eligible for a transition fill. That was wrong. 42 CFR §423.120(d) provides a coverage, transition, and exception pathway for compounds containing at least one Part D-qualifying ingredient. The same version described vaginal products approved for dyspareunia as structurally excluded from Part D; we found no evidence plans apply the exclusion that way, and corrected it. We also had the mid-year formulary notice period at 60 days; it’s 30. Corrected July 2026.
Who wrote this. Prepared by The HRT Index editorial team. This is editorial insurance research. It has not been medically reviewed by a clinician, and we’re not going to put a doctor’s name on it to make it look like it was. Found something wrong?Send us the source. We’ll fix it and date the correction. We don’t quietly swap facts.
Frequently asked questions
Does Medicare Part D cover estradiol patches?
Yes, when your plan lists your exact product. Coverage is decided product by product, so a weekly patch, a twice-weekly patch, and different strengths are separate decisions -- and two generic patches from different manufacturers are different products. Patches are where we see the most year-to-year churn, so recheck yours every January when your Annual Notice of Change arrives.
Does Medicare cover estradiol cream?
Often, but the tier and cost swing widely. Generic estradiol vaginal cream (Estrace) was 49.5% of all vaginal estrogen claims in Part D in 2016 and remains one of the most commonly listed products. Still: check your exact plan, because the cost difference between a preferred tier and a standard tier on the same drug can be significant.
Does Medicare Part D cover compounded or bioidentical HRT?
It depends what is in it. Under 42 CFR §423.120(d), a compound can be covered under Part D only if it contains at least one ingredient that independently meets the Part D drug definition. Part D then pays for those qualifying ingredients only. Compounds with no qualifying ingredient -- which includes most custom bi-est and tri-est creams made from bulk hormone powder -- are outside Part D entirely, and the exceptions process cannot be used for them (§423.578(e)). FDA-approved bioidentical products like estradiol patches and Prometrium are covered every day under the normal formulary rules.
Does Medicare cover hormone pellets?
Compounded pellets, including the BioTE-style kind, are not FDA-approved finished drugs. Whether Part D pays anything toward one depends on the exact product, its ingredients, how it is administered, whether Part B or Part D rules apply, and your plan's determination. Ask your plan for a determination in writing rather than trusting any website, including this one.
Does prior authorization mean I was denied?
No. Prior authorization means the plan wants clinical documentation before it decides. It is a paperwork step, not a rejection. Your prescriber submits it, and the plan has 72 hours to answer once it has the supporting statement -- 24 if expedited.
Can my doctor make Medicare cover a drug that is not on the list?
Often, yes, through a formulary exception. Under 42 CFR §423.578(b), the plan must grant it when it determines the drug is medically necessary consistent with your prescriber's statement and it would otherwise be covered. The statement has to say the covered alternatives on any tier would be less effective for you, would cause you adverse effects, or both. It can start as a phone call. But §423.578(f) is explicit that the statement does not guarantee approval -- the plan makes the determination.
What if my plan blows the 72-hour deadline?
You win a step automatically. Under §423.578(c)(2), the plan's failure to decide on time is itself an adverse determination, and the plan must forward your request to the Independent Review Entity within 24 hours. You do not file anything.
How long does an approved exception last?
The rest of the plan year. Under §423.578(c)(4), the plan cannot make you re-request approval for refills as long as your prescriber keeps prescribing it, it remains safe for you, and your enrollment period has not expired. The catch: if you renew for the next plan year, the plan may choose to continue coverage -- it is not automatic. Check your Annual Notice of Change in September.
Does the $2,100 cap make my HRT free?
Only for covered drugs. Once your out-of-pocket on covered Part D drugs hits $2,100 in 2026, you pay $0 for covered drugs the rest of the calendar year. Anything you paid with a discount coupon does not count, and neither do premiums.
Is it cheaper to pay cash with a coupon?
It depends on whether you would realistically hit the $2,100 cap. Coupon dollars do not move you toward your deductible or your cap. On an expensive drug you will take all year, that matters a lot -- the cap is your best protection and coupons do not get you there. On a cheap generic you would never spend $2,100 on, the cap is irrelevant and the coupon may just be cheaper. Do the math both ways for a full year. Under 42 CFR §423.120(a)(8)(iii), your plan cannot penalize your pharmacist for telling you the cash price is lower.
Why does my Veozah savings card not work on Medicare?
Because you have Medicare. Astellas' terms void the program for anyone whose claims are reimbursed by a state or federal program, and the list explicitly includes Medicare, Medigap, TRICARE, VA, and state assistance programs. Bayer's Lynkuet card carries the same restriction. Your replacement is the $2,100 cap -- which only helps if the drug is covered, which is exactly why the formulary exception is worth filing.
Will Medicare make me stop HRT at 65?
No. There is no age rule in Part D. On the medical side, The Menopause Society's 2022 position statement holds there is no general rule for stopping based on age alone, while the 2023 AGS Beers Criteria advise against initiating systemic estrogen in older women and suggest considering deprescribing. Both agree low-dose vaginal estrogen is appropriate. If you were denied and you are over 65, your age is not the cause -- find which of the four questions above applies.
Can I use my HSA to pay for HRT on Medicare?
You can spend an existing balance, but you cannot add to it. IRS Publication 969 is direct: beginning with the first month you are enrolled in Medicare, your HSA contribution limit is zero. Money already in your HSA stays yours and stays tax-free for qualified medical expenses.
Does Medicare Advantage cover more HRT than a stand-alone Part D plan?
Not inherently. An MA-PD plan uses a Part D formulary with the same rulebook -- tiers, restrictions, exclusions, exceptions. Every plan builds its own list, so a specific MA-PD might cover your patch when a specific PDP does not, or the reverse. Bundling the benefits onto one card does not change what is on the list. Some Medicare Advantage plans do not include drug coverage at all -- check yours.
Can an online menopause clinic write a prescription my Part D plan will cover?
Yes, if the clinician is licensed in your state and in good standing, the prescription is FDA-approved and on your formulary, and it goes to your own network pharmacy. The visit is cash either way -- no menopause telehealth service we have verified bills Medicare. But the drug is a separate transaction, and that is the one Part D pays for.
What to do next
The right next step depends on where you are right now. Find your row.
| Your situation | Do this |
|---|---|
| My pharmacy just rejected it | Work the four questions. Get the actual rejection reason, then build your exception packet. |
| I don't know if my drug is on my plan's list | Look it up in Plan Finder with the exact name, strength, and form |
| My compounded cream isn't covered | Ask the compounding pharmacy whether it contains any FDA-approved drug product. That answer decides everything. |
| My plan changed my drug in January | Ask for your transition fill today. Then file the exception. |
| My plan changed my drug mid-year | Say "current enrollee exemption." Ask where your 30-day notice was. |
| I might qualify for help paying | Check Extra Help — and answer SSA's burial-expense question truthfully |
| My doctor won't write the supporting statement | Ask why first. If the criteria genuinely aren't met, a second opinion is a real evaluation — not a signature you can buy. |
| I'm picking a plan for next year | Compare with your complete drug list, not just hormones |
| I don't know if online care is even right for me | Use the tool. Don't book anything yet. |
| Chest pain or possible heart attack symptoms | Call 911 now. Bleeding after menopause or a new breast lump — call your doctor today. This page is not for that. |
You are not being unreasonable. You’re not too old. And you’re not the only one—the number of Medicare women filling vaginal estrogen fell 72% in five years, for the one hormone product geriatric medicine actively recommends for women their age.
Most of them never heard the words “transition fill,” “formulary exception,” or “must grant.” You have now.
Still not sure which HRT path fits your situation?
Free. About 90 seconds. It matches your symptoms, your age, your route preference, your risk history, your insurance situation, and your state to the right path—and it will tell you when online care isn’t the right starting point.
Get my personalized HRT action plan →No email required to see your result
The HRT Index is reader-supported. Some links on this page are affiliate links, and we may earn a commission if you book through them at no additional cost to you. It doesn’t influence what we publish—the highest-paying partner in our stack is the one we spent this page explaining is structurally wrong for most Medicare beneficiaries.