The 30-second version, by situation
Find your row. The evidence behind each one follows below.
| Your situation | The short answer |
|---|---|
| Estrogen pills (oral, whole-body) | The strongest trial evidence showed a small rise in stroke risk. |
| Lower-dose transdermal estrogen (best studied as patches) | Studies have not shown that same rise — but “lower” is not “zero.” |
| You’ve had a stroke or TIA | Not a routine automated online-prescribing decision. Start with the clinician managing that history. |
| Vaginal estrogen (local) | Judge each product on its own. Early data on tablets is reassuring; rings and creams differ. |
| Using HRT to prevent stroke | No. Treating symptoms and preventing disease are two different decisions. |
This page is for you if
- You’ve been offered HRT and the word “stroke” scared you
- You’re weighing a pill against a patch, gel, or vaginal estrogen
- You’ve read “increased risk” and want to know what it means in real numbers
- You have migraine with aura, high blood pressure, or you’re over 60
- You saw the 2026 FDA warning news and don’t know what to believe
This page is not enough on its own if
- You might be having stroke symptoms now → call 911
- You’ve had a stroke or TIA → start with your vascular clinician
- You want to start, stop, or change a prescription today → talk to your prescriber
- You need your own personal risk number → only a clinician can estimate that
Not sure which situation is yours?Our free matching tool maps your symptoms, anatomy, route preference, and risk history to the right starting point in about 90 seconds — and flags honestly when you should see an in-person clinician first.
Find my HRT path →Heads up: Find My HRT Path may show telehealth providers we have an affiliate relationship with. If you start care through one, we may earn a commission — at no extra cost to you, and it never changes what this page tells you.
Does HRT increase stroke risk?
Some forms of HRT have been linked to a small rise in stroke risk, but “HRT” is not one single thing. The strongest randomized evidence involved two oral products, taken by mouth, in women whose average age was about 63. Route, dose, age, and your own health history all change how much that evidence applies to you.
The word “HRT” hides a lot of choices. It can mean a pill, a skin patch, a gel, a spray, or a vaginal tablet, ring, or cream. It can mean estrogen alone or estrogen plus a progestogen. It can be a low dose or a high one. Each of those choices changes the stroke question.
Four things move the answer more than anything else:
1
Whole-body vs. local
Whole-body (“systemic”) estrogen circulates everywhere. Local vaginal estrogen mostly stays where you put it.
2
Pill vs. skin
Swallowed estrogen (oral) behaves differently from estrogen absorbed through the skin (transdermal).
3
Dose and duration
How much, for how long. Higher doses and longer use each affect the picture.
4
You
Your age, your years since menopause, your blood pressure, and your vascular history.
What the big trials actually studied
The WHI hormone trials reported their main results in the early 2000s. They studied oral conjugated equine estrogens 0.625 mg daily (a form sold as Premarin), alone or with medroxyprogesterone acetate (MPA) 2.5 mg daily, in women ages 50–79 whose average age was about 63 — older than many women who start HRT for symptoms today. That detail matters: even if a treatment raises risk by the same percentage at every age, older women start from a higher baseline, so the same relative effect adds more real events.
Too simple: “all HRT causes strokes”
This lumps pills with patches, high doses with low, and 63-year-olds with 52-year-olds.
Also too simple: “modern HRT has no stroke risk”
“Lower risk” is not the same as “no risk.” That honest distinction matters.
The honest limitation
No study can give you a precise personal estimate of the stroke risk attributable to HRT. The strongest randomized evidence tested older, oral products — not the full range of low-dose patches, gels, and vaginal products women use now. That’s why this page separates what the trials found, what newer studies suggest, what labels require, and what only a clinician can decide for you.
How big is the stroke risk from HRT, in real numbers?
In current FDA labeling, the WHI oral estrogen-plus-MPA regimen was linked to 9 additional strokes per 10,000 women-years in the overall ages 50–79 group. Oral estrogen alone was linked to 11 additional strokes per 10,000 women-yearsoverall. In ages 50–59, the differences were +5 for combined therapy and −1 for estrogen alone, and both confidence intervals crossed 1. The excess was driven by ischemic stroke.
“Per 10,000 women-years” in plain terms
Ten thousand women-years could mean 10,000 women followed for one year, or 2,000 women followed for five years. It’s a population rate — not one reader’s personal annual chance.
Relative risk vs. real numbers
The combined oral regimen had an RR of about 1.37 — “37% more strokes.” But 37% more of a small number is still a small number: 9 extra per 10,000 women-years. “37% higher” and “9 more per 10,000” describe the same result. One sounds terrifying. One shows the absolute scale.
What a confidence interval tells you
A 95% confidence interval that crosses 1.0 means the study did not detect a statistically significant difference at the usual threshold. For the ages 50–59 combined-product group, the interval crossed 1.0 — so no one can hand a 52-year-old a precise stroke number from that subgroup.
The HRT Index Stroke-Risk Evidence Map — Part 1: What the randomized trials found (oral products, WHI)
These are the strongest kind of evidence — randomized trials — as reproduced in current FDA labeling.
| Oral WHI regimen | Age group | Stroke result (per FDA labeling) | Absolute rate | Difference | Certainty |
|---|---|---|---|---|---|
| CEE 0.625 mg + MPA 2.5 mg | 50–59 | RR 1.51 (95% CI 0.81–2.82) | 15 vs. 10 per 10,000 women-years | +5 | Not statistically significant |
| CEE 0.625 mg + MPA 2.5 mg | 50–79 | RR 1.37 (95% CI 1.07–1.76) | 33 vs. 24 per 10,000 women-years | +9 | Statistically significant |
| CEE 0.625 mg alone | 50–59 | RR 0.99 (95% CI 0.53–1.85) | 16 vs. 17 per 10,000 women-years | −1 | Not statistically significant |
| CEE 0.625 mg alone | 50–79 | RR 1.35 (95% CI 1.07–1.70) | 45 vs. 34 per 10,000 women-years | +11 | Statistically significant |
What the labels state: these rows report all-stroke results reproduced in current FDA labeling. Our reading: the overall groups showed a small, real increase; the younger subgroups were regimen-specific and imprecise. The limitation:these oral, standard-dose products from the early 2000s do not automatically describe low-dose patches, gels, or vaginal products. Note also that in ages 50–59 groups, the placebo stroke rates were 10 per 10,000 women-years (combined trial) and 17 per 10,000 (estrogen-alone trial) — trial-specific rates, not a universal baseline.
Now the useful part: which of those rows is about you?
You know the size of the risk and its limits. What you don’t know yet is which situation describes you. Build your clinician question list ↓ — a private, printable set of questions matched to your route, age, and history. It won’t give you a risk score, but it will make your appointment count.
See which care path fits →Is stroke the same as a blood clot?
No. “Blood clot” usually means a clot in a vein — a deep-vein thrombosis (DVT) in the leg or a pulmonary embolism (PE) in the lungs. Most strokes discussed with HRT are events in an artery in the brain. They share some risk factors, but the evidence and the size of the risk are different, so the two shouldn’t be treated as one.
Venous events (clots in veins)
DVT (usually in the leg), PE (clot that travels to the lungs). The umbrella term is VTE — venous thromboembolism.
Arterial events (in arteries)
Ischemic stroke (a blocked artery in the brain), hemorrhagic stroke (a bleed in the brain), and TIA — a transient ischemic attack, a temporary episode of stroke-like symptoms that still needs urgent medical assessment.
| Outcome type | Strongest route signal | The mechanism | The inference you can’t make |
|---|---|---|---|
| Venous clot (DVT/PE) | Oral higher than transdermal in observational studies | Oral estrogen’s first pass through the liver affects clotting markers | That skin routes carry zero clot risk |
| Arterial (ischemic stroke) | Oral higher than transdermal in observational studies | Same first-pass mechanism, plus vascular factors | That a lower observed rate proves cause, or zero risk |
Transdermal estrogen avoids first-pass hepatic metabolism and generally has less effect on the liver’s clotting markers than oral estrogen. That’s a plausible mechanism — a reason — not proof of zero clinical stroke risk. See also: HRT and blood clots.
Is a patch safer than pills for stroke risk?
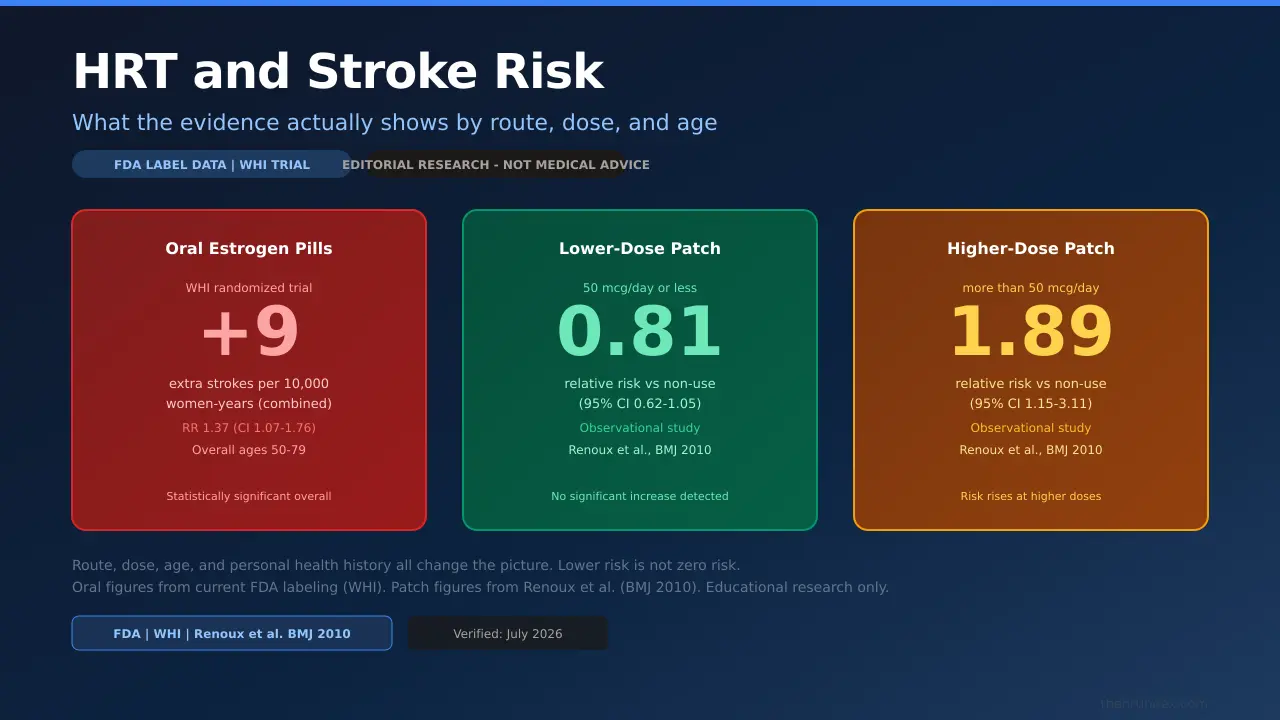
For stroke risk, the route matters. Lower-dose transdermal estrogen — best studied as patches — has generally notshown the rise in stroke risk seen with pills in observational studies. In one large study, current oral HRT was linked to about 28% higher stroke risk than non-use, while current transdermal HRT was not linked to a significant increase. But higher-dose patches (over 50 mcg/day) did show a rise, so “patch” alone doesn’t mean “safe.”
Transdermal means estrogen absorbed through the skin — a patch, a gel, or a spray — instead of swallowed. Because it skips the first pass through the liver, it doesn’t push the liver’s clotting markers the same way a pill does. Note that the strongest direct stroke-outcome evidence is for patchesspecifically; gels and sprays are transdermal too, but they don’t each have the same dedicated stroke-outcome data.
The HRT Index Stroke-Risk Evidence Map — Part 2: Route, dose, and local products
Mostly observational studies. Observational studies can spot patterns, but they can’t prove cause the way a randomized trial can.
| Situation | Type of evidence | Result | What it supports | What it does NOT support |
|---|---|---|---|---|
| Current oral HRT vs. non-use | Observational | RR 1.28 (95 CI 1.15–1.42) | Oral linked to a higher stroke rate than non-use | "Every pill raises every woman’s risk by 28%" |
| Current transdermal HRT overall vs. non-use | Observational | RR 0.95 (95 CI 0.75–1.20) | No significant increase detected | "Patches have zero stroke risk" |
| Lower-dose patch (≤50 mcg/day) | Observational | RR 0.81 (95 CI 0.62–1.05) | No significant increase at lower doses | "Proven safe for everyone" |
| Higher-dose patch (>50 mcg/day) | Observational | RR 1.89 (95 CI 1.15–3.11) | Risk can rise at higher doses, even through the skin | "All patches are safe at any dose" |
| Oral vs. transdermal (direct comparison) | Systematic review; stroke estimate from one case-control study | RR 1.24 (95 CI 1.03–1.48) | Suggests higher stroke risk with oral therapy | A replicated, high-confidence pooled result across many stroke studies |
| Vaginal estradiol tablets, after prior ischemic stroke | 2025 nationwide observational study | No significant association; current-use aHR 0.79 (95 CI 0.52–1.20) | Tablet-specific, reassuring in this group | Proof of protection; does not cover creams or rings |
What the guidelines say: The Menopause Society states that transdermal routes and lower doses maydecrease the risk of stroke and blood clots. Read that carefully — it’s a careful “may,” backed by observational data, not a guarantee. That’s the honest state of the evidence, and it’s still genuinely useful for anyone weighing a pill against a patch.
Does the dose change the risk too?
Yes — dose appears to matter, especially for pills. UK guidance (NICE NG23) distinguishes regimens: for oral estrogen-only HRT, stroke risk rises with dose and with older age at starting; for oral combined HRT, it rises with dose, duration, and older age at starting. Even patches showed a higher rate at higher doses in one study. Lower effectivedoses are generally preferred when stroke risk is a concern — but “effective” is the key word, because a dose too low to control your symptoms isn’t a win. That balance is a clinician’s call, not a self-adjustment.
Do not change your own treatment based on this. Don’t cut patches, change your dose, swap to a gel, or stop your progestogen on your own. Route and dose are a conversation with your prescriber.
Does age or time since menopause change HRT stroke risk?
Age and timing change the baseline your risk sits on. For healthy women under 60, or within 10 years of menopause, the benefit-to-risk balance is generally more favorable. For women who start HRT more than 10 years from menopause onset, or after age 60, the balance is generally less favorable — because the underlying risks of coronary disease, stroke, venous clots, and dementia are higher to begin with. These are not simple safe/unsafe cutoffs, and they don’t override your personal history.
Why "younger" usually means lower absolute risk
Even if a treatment raises risk by the same percentage at every age, the same percentage of a smaller baseline is a smaller number of actual strokes. Younger women start from a lower baseline, so the same relative effect adds fewer real events.
What "within 10 years" actually means
It's counted from menopause onset — usually dated from your final menstrual period, once 12 months have passed with no period. Surgical menopause is dated from the surgery. Perimenopause can blur that date, so if you’re not sure where you land, that’s a question for your clinician — not a reason to guess.
What changes after 60
Don’t read "after 60" as "banned." What’s true is that everyday vascular risk rises with age, and starting HRT later is a different question from continuing an established, tolerated regimen. Older age at the first prescription is where clinicians look harder at route, dose, and your overall heart-and-vessel health.
Early or premature menopause is different
Women who reach menopause early may face higher risks from low estrogen and are often advised to use hormone therapy until at least the typical age of natural menopause, unless a contraindication applies. If that’s you, it’s a distinct conversation — bring it up directly.
Your situation: an HRT & stroke question builder
Turn the evidence into yourquestions. Answer a few things — your route (or the one you’re considering), your age range, your time since menopause, and any history like a past stroke, TIA, migraine with aura, or high blood pressure — and we’ll build you a list to bring to your appointment.
Your route or the one you’re considering
- Pills / oral estrogen
- Patch / gel / spray
- Vaginal estrogen only
- Not sure yet
Age range
- Under 50
- 50–59
- 60 or older
- Premature / early menopause
History flags
- Past stroke or TIA
- Migraine with aura
- High blood pressure
- Blood clot (DVT/PE)
Your answers stay on your device. We don’t ask for your email. Educational only — not medical advice or a personal risk assessment. See our consumer health data privacy page.
What it will not do:give you a risk percentage, diagnose you, or tell you a route is “safe” for you. Those are a clinician’s job. This helps you walk in prepared with the questions and records that need to be addressed.
Can you take HRT after a stroke or a TIA?
A past stroke or TIA is not a routine, automated online HRT decision. Current U.S. prescribing information for many whole-body (systemic) estrogen products lists a history of stroke as a reason not to use them. Whether any hormone therapy — including low-absorption vaginal estrogen — is an option depends on your stroke type, its cause, and your current care, and it should be decided with the clinician who manages your vascular health.
If you’ve had a stroke or a TIA, the general evidence above is not enough on its own. Here’s why.
What U.S. labels say (selected examples, not the whole market)
| Product (examples) | Type / route | Prior-stroke status in current U.S. label |
|---|---|---|
| Bijuva | Systemic — oral estradiol + progesterone | Lists active or prior arterial thromboembolic disease (such as stroke) as a contraindication |
| Enjuvia | Systemic — oral synthetic conjugated estrogens | Lists active or previous stroke as a contraindication |
| Estring | Vaginal ring — local, low-dose | Retains the prior-stroke contraindication despite lower systemic exposure |
Why the cause matters so much
A clinician may need to know whether your stroke was ischemic (a clot) or hemorrhagic (a bleed), whether it was a TIA or a completed stroke, whether an irregular heartbeat (atrial fibrillation) was involved, what blood thinners you take, and how your blood pressure is controlled. A generic automated intake form alone cannot resolve those issues.
Why UK advice can sound more open
UK guidance supports an individualized post-stroke assessment. That can be reasonable in the right hands — but U.S. prescribing decisions must follow the label of the specific U.S. product, and UK guidance does not override a U.S. product contraindication. Both things are true; the U.S. label sets the U.S. rule.
Bring these to your appointment
- Your hospital discharge or neurology summary
- Your stroke type and date
- Your full medication list, including blood thinners
- Your blood-pressure history
- The menopause symptoms you want treated
- The exact product or route being considered
Important
Do not start, restart, stop, or change systemic HRT after a stroke or TIA based on this page. Begin with the clinician who manages your vascular or neurological health. See also our HRT contraindications guide.
Does vaginal estrogen increase stroke risk?
Vaginal (local) estrogen is not one product or one dose. A 2025 nationwide study of women who had already had a stroke found no significant association between vaginal estradiol tabletuse and a repeat stroke. But that study looked at tablets — not every cream or ring — and some product labels (like the Estring vaginal ring) still list a history of stroke as a contraindication despite lower absorption.
Local vs. whole-body
Local vaginal estrogen treats vaginal and urinary symptoms — dryness, pain with sex, urgency — a cluster doctors call the genitourinary syndrome of menopause (GSM). Systemic exposure is generally lower than with whole-body therapy, but absorption varies by product, dose, and time after starting.
Why product specifics matter
The 2025 reassuring data was for vaginal estradiol tablets specifically. Creams, rings, and different dose formulations each have their own absorption profiles. A low-dose local ring (like Estring) and a systemic ring (Femring) are entirely different products with different risk profiles. Don’t assume one product’s data covers another.
Still check the specific label
Even with lower systemic exposure, some local vaginal products retain prior-stroke as a contraindication in their current U.S. prescribing information. Ask your prescriber about the specific product, its label status, and whether it’s appropriate given your history.
Special situations: migraine with aura, high blood pressure, hysterectomy
Migraine with aura
Migraine with aura is not treated as an automatic barrier to menopausal HRT. UK guidance from the British Menopause Society (April 2026) says aura does not contraindicate menopausal HRT and recommends non-oral estradiol at the lowest effective dose. That’s different from the birth control pill’s aura warnings — the mechanisms and hormone levels are different. New or unusual neurological symptoms still need urgent review, and factors like blood pressure and smoking still matter on top of the aura history.
High blood pressure
Controlled high blood pressure is not automatically a contraindication, but your blood pressure should be assessed — and uncontrolled high blood pressure addressed — before starting whole-body treatment. Route and other vascular risks still matter on top of that. See also: hrt-and-high-blood-pressure.
Hysterectomy
A hysterectomy can change whether you need endometrial protection, so you may be a candidate for estrogen alone — but it does not automatically remove the estrogen-related stroke question. Route, dose, age, and vascular history still matter. And a partial (supracervical) hysterectomy or a prior endometrial ablation changes the picture further.
See also: HRT and migraine with aura · HRT and high blood pressure · HRT and heart disease
What the 2026 FDA label change actually means for stroke risk
The FDA did not say that HRT no longer causes stroke. In November 2025, the FDA requested removal of cardiovascular disease, breast cancer, and probable-dementia statements from the menopause hormone therapy boxed warning. The first six updated product labels were approved February 12, 2026. Cardiovascular risk information remained in the labeling itself, and many products still list prior stroke as a contraindication. The boxed warning changed; the underlying risk question did not disappear.
What changed
The FDA removed cardiovascular, breast cancer, and probable-dementia bullet points from the headline boxed-warning section of select menopause hormone labeling. This reflects a reassessment of the evidence, particularly for younger women closer to menopause onset.
What did not change
Cardiovascular risk discussion remains in the labeling body. Many products still list prior stroke as a contraindication. The WHI stroke data still exists and still applies to the specific oral products it studied. Labels continue to be updated product by product.
What it means for you
Check the current label of the specific product you are considering or using. The labeling update applies to products that were updated; it does not retrospectively change what the WHI found, and it does not mean all stroke risk has been removed from all products.
What women actually ask about HRT and stroke risk
These reflect the real questions and fears that bring women to this page. They show what women are trying to resolve — they are not medical evidence and don’t establish anyone’s outcome.
- Having a prescription in hand but feeling too afraid to start because of the stroke warning on the insert
- Not knowing what “increased risk” means in absolute numbers
- Getting conflicting recommendations from different clinicians or sources
- Wondering whether a patch really changes anything, or whether it’s just marketing
- Wondering what happened to the stroke risk after the FDA update in 2026
- Wanting to know if a prior blood clot means they can’t take anything
- Needing to know what to do if they’ve already had a stroke and their symptoms are bad
Fair questions, all of them. That’s the whole reason for the numbers, the route comparison, and the question builder above.
What we actually verified
For this page, our team checked the FDA’s November 2025 labeling action and the February 2026 label approvals, current U.S. prescribing information, the Women’s Health Initiative (WHI) stroke figures as reproduced in current labeling, The Menopause Society’s 2022 position statement, and route-and-dose studies from peer-reviewed journals. We did not test any medication, calculate anyone’s personal risk, or have a clinician review this page. The accuracy is ours to own; errors should be reported to our corrections page.
| Source | Year | What it covers on this page |
|---|---|---|
| Women's Health Initiative hormone trials (oral estrogen data reproduced in current FDA labeling) | 2002–current | Oral WHI stroke figures used throughout |
| FDA menopausal hormone therapy labeling action (boxed warning) | Nov 2025 / Feb 2026 | 2026 FDA label change section |
| The Menopause Society 2022 position statement | 2022 | Transdermal route guidance; timing window |
| Renoux et al., BMJ 2010 — "Transdermal and oral hormone replacement therapy and the risk of stroke" | 2010 | Route and dose evidence map (Part 2) |
| 2025 nationwide observational study — vaginal estradiol tablets and recurrent ischemic stroke | 2025 | Vaginal estrogen section |
| Fournier et al. — progestogen class and stroke (French cohort) | 2016 | Micronized progesterone FAQ item |
| NICE menopause guideline (NG23) | 2024 update | Dose/duration dose-risk section; age guidance |
| British Menopause Society — migraine and HRT guidance | Apr 2026 | Migraine with aura section and FAQ |
| USPSTF — hormone therapy for primary prevention | Current | Prevention vs. symptom treatment context |
| ACOG — compounded bioidentical hormone therapy / pellets | Current | Compounded HRT FAQ item |
What this page can’t do: give you a personal risk number; point to a single head-to-head trial of every modern route and dose; promise labels won’t change; reconcile every difference between U.S. and UK guidance for your case; or replace a clinician who can review your history, medications, blood pressure, records, and any relevant testing. See our corrections page for any updates.
Frequently asked questions
Does HRT increase your risk of stroke?
Some forms do, slightly. In current FDA labeling, oral estrogen-plus-MPA was linked to about 9 additional strokes per 10,000 women-years overall, and oral estrogen alone to about 11 additional per 10,000 women-years overall; the excess was driven by ischemic stroke. Lower-dose transdermal estrogen (best studied as patches) has not shown that same rise in observational studies. Your route, dose, age, and history all change how much this applies to you.
Which HRT has the lowest stroke risk?
There is no single lowest-risk HRT for everyone. Lower-dose transdermal estrogen, best studied as patches, is generally favored over pills when stroke or clot risk is a concern, and local vaginal estrogen has lower systemic exposure. Personal history, dose, symptoms, and uterus status still matter, so this is a clinician conversation.
Is an estrogen patch safer than pills for stroke risk?
For stroke and clot risk, the skin route has generally looked more reassuring than pills in observational studies. One large study found no significant stroke increase with transdermal versus about 28% higher with oral, each compared to non-use. But lower risk is not zero risk, and higher-dose patches over 50 mcg/day showed a rise. It is a meaningful difference, not a guarantee.
Can you take HRT after a stroke or TIA?
This is not a routine automated online decision. Many U.S. systemic estrogen products list prior stroke as a contraindication, and whether any option, including low-absorption vaginal estrogen, is appropriate depends on your stroke type, cause, and current care. Start with the clinician who manages your vascular health.
Does vaginal estrogen increase stroke risk?
Local vaginal estrogen has lower systemic exposure, and a 2025 study found no significant association between vaginal tablet use and a repeat stroke among women who had already had one. But that was tablets specifically, it was observational, and some product labels such as Estring still list prior stroke. Ask about the specific product.
Is HRT safe if you have migraine with aura?
Migraine with aura is not treated as an automatic barrier to menopausal HRT; UK BMS guidance says aura does not contraindicate it and recommends non-oral estradiol at the lowest effective dose. That differs from the birth control pill aura warnings. New or unusual neurological symptoms still need urgent review, and blood pressure and smoking matter.
Can you start HRT after age 60?
Age 60 is not a hard prohibition, but starting later generally calls for a closer look at timing, baseline vascular health, route, dose, and reason for treatment. Do not read under 60 or within 10 years as an automatic yes or no; it is a starting point for the conversation.
Can you use HRT with high blood pressure?
Controlled high blood pressure is not automatically a contraindication, but blood pressure should be assessed and uncontrolled high blood pressure addressed before starting whole-body treatment. Route and other vascular risks still matter on top of that.
Does having a hysterectomy change HRT stroke risk?
A hysterectomy can change whether you need endometrial protection, so you may be a candidate for estrogen alone, but it does not automatically remove the estrogen-related stroke question. Route, dose, age, and vascular history still matter, and a partial hysterectomy can change the picture.
Does micronized progesterone remove the stroke risk?
No. The type of progestogen may matter, and a 2016 study found micronized progesterone was not linked to a significant stroke increase while some synthetic progestogens were, but that is observational and does not prove any option removes risk. With a uterus and whole-body estrogen, you generally still need endometrial protection.
Can aspirin or a blood thinner make HRT safe?
No, and do not change those medicines on your own to offset HRT risk. Aspirin, antiplatelets, and anticoagulants have their own reasons for use and their own bleeding risks; the clinician managing them must decide how they affect any hormone-therapy discussion.
Did the FDA say HRT no longer causes stroke?
No. In November 2025 the FDA requested the boxed-warning change, and the first six updated product labels were approved on February 12, 2026, but cardiovascular risk information stayed in the labeling and many products still list prior stroke as a contraindication. The presentation changed; the underlying risk question did not disappear.
Should you stop HRT because you are afraid of stroke?
Do not make a non-emergency medication change based on an article. Call your prescriber to discuss your exact product, route, dose, symptoms, and history, and call 911 for any possible stroke symptoms happening now.
Still deciding?
Still not sure which HRT program is right for you? Take our free 90-second matching quiz — Find My HRT Path — and get your personalized next-step plan, including a flag for when to start with an in-person clinician.
Take the free quiz →The HRT Index provides educational editorial research. This page is not medical advice. If you may be having stroke symptoms, call 911.