On this page
- Five things that determine the answer
- Why isn’t there an FDA-approved testosterone for women?
- What “compounded” actually means — and who checks it
- What testosterone is actually proven to do for women
- Are testosterone pellets safe for women?
- Which side effects reverse — and which don’t?
- Can testosterone cream transfer to a partner or child?
- Already taking it? Here’s what to do this week
- How would you know if your dose is too high?
- Is compounded testosterone safer than a men’s product?
- What to check before you fill it
- Who should not start this online
- Who actually prescribes testosterone to women
- Does “bioidentical” mean safer?
- How long can a woman safely take testosterone?
- Will you still be able to get this in 2027?
- How this page was verified
- Frequently asked questions
Five things that determine the answer
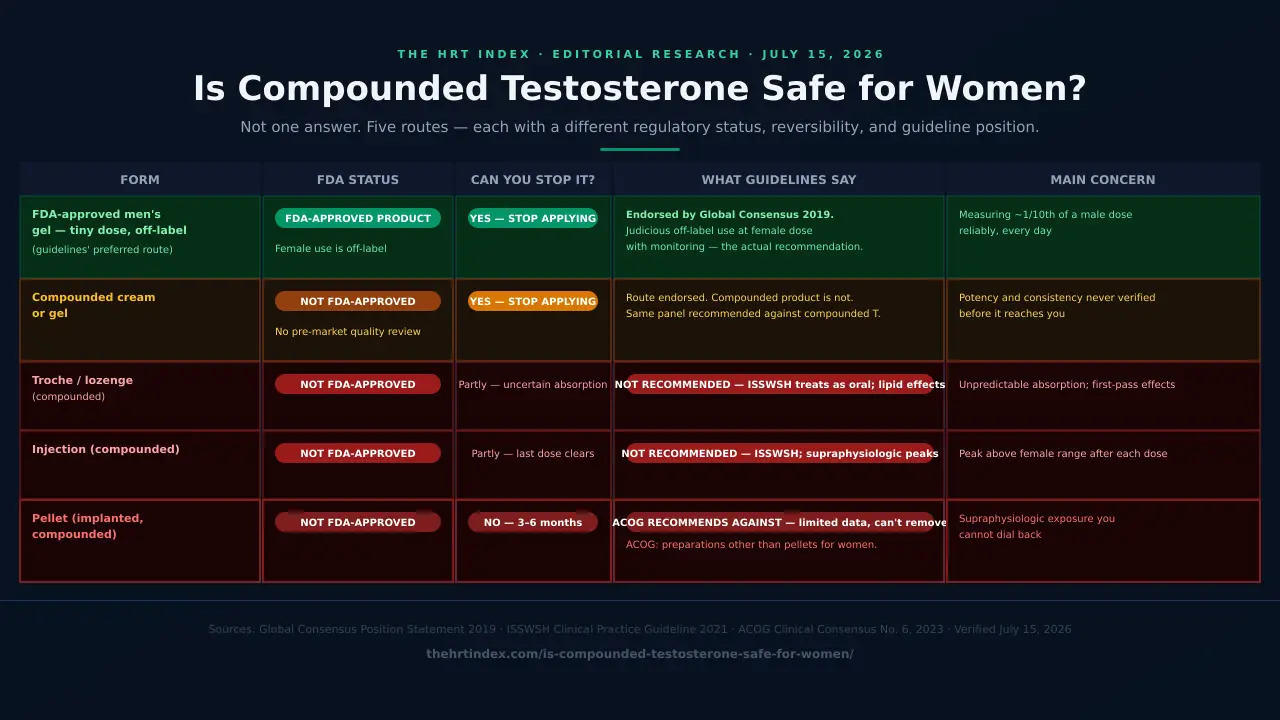
“Is compounded testosterone safe for women?” is five questions wearing one coat. The form, the dose, whether you can stop it, whether the product was ever checked, and whether anyone is monitoring you all produce different answers — and they produce very different risk profiles when combined wrong.
| Question | Why it matters | What makes it safer | What makes it riskier |
|---|---|---|---|
| What form? | Route changes bioavailability, reversibility, and guideline position | Topical (cream, gel) — endorsed route. Apply, stop if needed. | Pellet — ACOG recommends against. Not designed to come out. |
| What dose? | Above the female reference range, the documented failure modes appear | Physiologic female dose, checked against your lab’s premenopausal upper limit | Supraphysiologic — common with pellets; seen in potency-variable compounded products |
| Can you stop it? | Reversibility determines whether a wrong dose is a setback or a situation | Topical: yes. Stop applying. | Pellet: no practical stop button. 3–6 months of whatever dose you got. |
| Was the product checked? | No compounded drug is FDA-approved. Potency varies. | Pharmacy does finished-product potency testing and provides documentation | Raw-ingredient certificate only. No finished-product test. Nobody knows the actual concentration. |
| Is anyone monitoring you? | Symptoms are a late signal. Blood levels catch overexposure before you can see it. | Baseline labs, repeat at 3–6 weeks, scheduled follow-up every 4–6 months once stable | No baseline. No follow-up. “Your labs looked fine” with no number provided. |
Why isn’t there an FDA-approved testosterone for women?
The one submitted was rejected — not because it didn’t work, but because long-term safety data were absent. The advisory committee voted 14–3 that the benefit was clinically meaningful, then voted unanimously against approval. The safety trial built to close that gap was completed in 2012 and never published. Four other countries have since approved a 1% testosterone cream for women. The United States has approved nothing.
December 2, 2004: the vote that created this market
Procter & Gamble submitted Intrinsa, a testosterone patch for postmenopausal women with HSDD. The FDA’s advisory committee voted 14–3 that the benefit was clinically meaningful. Then they voted unanimously against recommending approval— because there wasn’t enough long-term safety data on breast cancer, cardiovascular outcomes, and other serious concerns.
The product that lost that vote was an FDA-reviewed, controlled-dose, properly manufactured patch. What filled the market after that rejection was compounded preparations — products the FDA hadn’t reviewed at all.
Source: FDA panel rejects testosterone patch for women on safety grounds. BMJ. 2004.
The LibiGel story
BioSante Pharmaceuticals ran the safety trial the FDA asked for. LibiGel was a topical testosterone gel for women. The trial was completed in 2012. It was never published.
A 2026 evidence review by the BC Provincial Academic Detailing Service records the trial as completed but unpublished. The gap the 2004 committee flagged remains open.
Four countries said yes. The U.S. said nothing.
| Country | Approved? | Regulator | Authorized | Notes |
|---|---|---|---|---|
| Australia | Yes — AndroFeme 1 cream, 10 mg/mL | TGA | 2020 | Registered for postmenopausal HSDD. Doesn’t affect U.S. status. |
| New Zealand | Yes — AndroFeme | Medsafe | Licensed | Regulator-listed for postmenopausal HSDD. |
| South Africa | Yes — TestaFeme | SAHPRA | Licensed | Regulator-listed. |
| United Kingdom | Yes — AndroFeme 10 mg/mL | MHRA | 25 July 2025 | Prescription-only marketing authorization. Authorization is not availability — check formulary and NHS access separately. |
| United States | No. None. | FDA | — | Intrinsa rejected 2004. Nothing approved since. |
Verified July 2026 via Lawley Pharmaceuticals and regulator listings.
Is anything coming?
Aviva Bio publicly reported a January 2026 FDA Type B meeting about the development pathway for its investigational product, AVA-291. Source: Aviva Bio company announcement (January 2026)— not an FDA statement, not approval. A Type B meeting is an early development milestone. Worth watching. Not worth waiting for.
The American situation: an Australian woman with your exact symptoms gets a licensed, batch-tested, regulator-reviewed 1% testosterone cream with a real label. You get a compounded cream, an approved men’s product used off-label, or nothing. The U.S. never resolved the safety question, never approved a product, and left a gap that compounding pharmacies stepped into — and a compounded product is one the FDA never reviewed before it reached you.
What “compounded” actually means — and who checks it
A compounded drug is mixed for one patient by a pharmacy instead of manufactured under FDA approval. The FDA’s position: compounded drugs are not FDA-approved, which means the agency does not verify their safety, effectiveness, or quality before they’re marketed. That isn’t the same as no oversight — the FDA can inspect, investigate, recall, and take enforcement action. What’s missing is the check that happens before the product reaches you.
Source: FDA — Compounding and the FDA: Questions and Answers.
Three words that get blurred constantly
| Word | What it means | What it does NOT mean |
|---|---|---|
| FDA-approved | The finished product went through an approval process. Manufacturing, labeling, release testing, and evidence were reviewed before sale. | That it’s approved for you, or for women. |
| Off-label | An FDA-approved product used outside its approved labeling — different condition, population, or dose. Legal, common, and often good medicine. | That the FDA approved it for that use. |
| Compounded | A pharmacy prepared it for a prescription. The finished product was never FDA-approved. | Not the same as “off-label.” Off-label describes an approved product used differently. A compounded product isn’t approved at all — a different regulatory category, not a stricter version of the same one. |
| Bioidentical | A hormone chemically identical to one your body makes. | Anything about FDA approval, manufacturing quality, correct dosing, effectiveness, or safety. There is no FDA category called “bioidentical.” |
503A vs. 503B: which rulebook applies to yours?
| 503A — traditional compounding pharmacy | 503B — registered outsourcing facility | |
|---|---|---|
| Premarket FDA approval | No | No |
| Patient-specific prescription required | Yes | Not necessarily |
| Primary regulator | State board of pharmacy | FDA, plus states |
| Current good manufacturing practice | Not held to the same requirements as a manufacturer | Required |
| Risk-based FDA inspection | Not routine | Yes |
| Mandatory federal adverse-event reporting to FDA | Generally no | Yes |
Source: FDA — Information for Outsourcing Facilities.
Ask which one made yours.It’s a fair question, takes one sentence, and the answer tells you which rulebook applies to the thing you’re putting on your skin every morning. When a website says “FDA registered,” ask which one it means — registration is not approval of anything.
If something goes wrong, who finds out?
A 503B outsourcing facility must report qualifying adverse events to the FDA. A traditional 503A pharmacy generally does not carry the same federal mandatory-reporting duty. But there is a channel almost nobody uses: you can report an adverse event or a product-quality problem yourself, through FDA MedWatch.Patients can file directly. You don’t need anyone’s permission.
Somebody did check the dose. Once. Here’s what they found.
In 2015, researchers sent a standardized testosterone prescription to ten Toronto-area compounding pharmacies and collected two independently compounded batches from each, one month apart— then measured by mass spectrometry.
- First set of samples: 50% of pharmacies were within ±20% of the prescribed concentration.
- Second set: 30% were.
- The FDA-approved comparison products in the same experiment — AndroGel and Testim — were accurate and consistent.
What those numbers mean — and what they can’t
In the second set of samples, seven of ten pharmacies supplied a product outside ±20% of what the prescriber wrote. Same prescription. Blinded. Measured by machine. This was 2015, in Canada, at ten pharmacies. It does notestimate the current failure rate for U.S. female-dose testosterone prescriptions, and it doesn’t tell you anything about your pharmacy. But it does tell you something you can’t un-know: “my dose is 5 mg” is a sentence that, in the only study designed to check it, was frequently not accurate.
What is testosterone actually proven to do for women?
The only evidence-based indication for testosterone in women is hypoactive sexual desire disorder in postmenopausal women, diagnosed after a full biopsychosocial assessment. The 2019 Global Consensus Position Statement — endorsed by The Menopause Society, the Endocrine Society, and the International Menopause Society — found the evidence does not support testosterone for any other symptom or condition in women. That includes energy, cognition, muscle, bone, mood, and cardiovascular health.
What it’s sold for vs. what the evidence shows
| What you were told it would do | What the evidence says | Source |
|---|---|---|
| Low sexual desire that distresses you, after menopause (HSDD) | Supported. Improves desire, arousal, orgasm, and pleasure; reduces sexual distress. The one recognized indication. | Global Consensus 2019; Islam RM et al. Lancet Diabetes Endocrinol. 2019 |
| Energy / fatigue | Not established | Global Consensus 2019 (evidence insufficient) |
| Cognition / “brain fog” | Not established | Global Consensus 2019 |
| Muscle mass or strength | Not established | Global Consensus 2019 |
| Mood / depression | Not established | Global Consensus 2019 |
| “Anti-aging” / “hormone optimization” | Not established. No testosterone deficiency syndrome in women has ever been defined. | Global Consensus 2019 |
| “Your blood test showed low T” | That test can’t do that. No cutoff for any circulating androgen separates women with sexual dysfunction from women without it. | Global Consensus 2019 |
| “We’ll use saliva testing to set your dose” | No. Adjunct hormone tests aren’t recommended for prescribing or dosing compounded hormones. | ACOG Clinical Consensus No. 6, 2023 |
Professor Susan Davis of Monash University led the 2019 Global Consensus Position Statement. At The Menopause Society’s 2025 Annual Meeting in Orlando, she told the room there is no justification for giving testosterone to women to protect muscle, prevent fractures, prevent heart disease, or treat depression, cognitive decline, or fatigue: “It is not the silver bullet; it is not the missing hormone.”
Davis SR. “Androgens for muscles, mood, and more.” The Menopause Society 2025 Annual Meeting, October 21–25, 2025, Orlando, FL.
What “it works” actually means, as a number
Across the relevant randomized trials, testosterone produced an average of about 0.85 additional satisfying sexual events per month compared with placebo or comparator. Not quite one a month.
We’re publishing that on purpose. Some women read it and think that’s it? Some read it and think one more a month would change my marriage.Both are legitimate, and it’s your call, not ours. But you can’t make that call if nobody gives you the number — and you probably weren’t given the number.
Are testosterone pellets safe for women?
ACOG recommends using preparations other than pellets to deliver testosterone to women, citing limited safety data and the inability to remove a pellet in routine practice. A 2021 study of 539 postmenopausal women found side effects in 57.6% of women on compounded pellet hormone therapy versus 14.8% of women on FDA-approved hormone therapy. The clearest, least arguable point stands on its own: a pellet is the one form that isn’t designed to come back out.
The pellet problem, in one sentence
It isn’t designed to come out.
That’s the whole thing. The convenience — four months, one appointment, no daily cream — is bought with that sentence. A pellet is a small compressed cylinder pushed under the skin, usually near the hip. It releases over roughly three to six months. There’s no dial and no pause. If exposure runs higher than intended, your realistic options are to wait it out or to discuss procedural retrieval with your clinician — which is a procedure with its own tradeoffs, not a stop button.
Compare that to a topical. Wrong dose? Stop applying it. That’s not a small difference. It’s the difference between a mistake and a situation.
The numbers, and exactly what they do and don’t show
| What was measured | Result | Study |
|---|---|---|
| Any side effect — compounded pellet hormone therapy vs. FDA-approved hormone therapy | 57.6% vs. 14.8% (221/384 vs. 23/155). Odds ratio 8.0 (95% CI 4.5–14.2), p<0.00001 | Jiang X et al. Menopause. 2021;28(8):867–874. 539 postmenopausal women. |
| Abnormal uterine bleeding in women with a uterus | 55.3% vs. 15.2% (136/246 vs. 12/79). Odds ratio 7.9 (95% CI 3.6–17.0) | Same study |
| Also significantly more common in the pellet group | Anxiety · breast pain · acne · hair-pattern changes · weight gain · need for hysterectomy · mammogram findings BI-RADS 4 or higher | Same study |
Two caveats, stated in full
First: This is compounded pellet hormone therapy, not isolated testosterone pellets. You cannot attribute that gap specifically to testosterone, to the pellet route by itself, or to any single hormone. Second: It’s a retrospective chart review, not a randomized trial. Women who choose pellets may differ from women who don’t in ways that affect the result. What it does is put an actual number on a gap — 57.6 against 14.8, in 539 real women — and pair it with the one thing that needs no statistics at all: you can’t take it back.
The company that sells testosterone and refuses to sell you a pellet
Midi Health prescribes compounded testosterone cream to women. They also don’t offer pellets, and they say so on their own site: a pellet can deliver more testosterone than intended, and once it’s implanted the treatment can’t be paused.
Sit with that. A telehealth company that could bill you for a procedure is publicly telling you not to buy one. Weigh that against whoever is currently offering you one.
Which side effects reverse — and which ones don’t?
In short-term randomized trials using physiologic female doses, the effects seen most consistently were mild acne and increased hair growth. ACOG states that hirsutism, acne, and virilization — which includes voice deepening and clitoral enlargement — may be irreversible. Excessive exposure and longer duration raise the concern, but reversibility cannot be predicted for an individual.
| What can happen | Might it reverse? | What kind of evidence |
|---|---|---|
| Oily skin, acne | Often improves when exposure comes down. ACOG: may be irreversible in some cases. | Seen consistently in randomized physiologic-dose trials |
| More body or facial hair (hirsutism) | Often improves, but hairs that have already coarsened don’t un-coarsen. ACOG: may be irreversible. | Seen consistently in randomized physiologic-dose trials |
| Scalp hair thinning (androgenic alopecia) | May improve. May not. | Guideline warning; midlife hair loss has many causes |
| Voice deepening | May be permanent. | Guideline warning + published case series |
| Clitoral enlargement (clitoromegaly) | May be permanent. | Guideline warning. Same. |
| Long-term breast cancer and heart risk | Not established. | Randomized data don’t extend far enough. Not “safe.” Not “risky.” Not established. |
The voice question, answered properly
The reassuring half: In short-term randomized trials using physiologic female exposure, there was no excess of voice change or clitoral enlargement.That’s a real finding and you should have it.
The half that should change what you watch for: A case series published in 2020 (Journal of Voice, online 2020, print 2021), from Weill Cornell and UT Health San Antonio, described nine women, average age 55, who turned up at voice clinics after taking testosterone. Three were professional performers. Most were on subcutaneous pellets. Onset ranged from immediately to 48 months, averaging 15 months. The authors concluded voice changes may be permanent.
Fifteen months
That’s the average gap between starting and showing up at a voice clinic. This isn’t a side effect that raises its hand in week two while it’s easy to fix. It arrives after you’ve decided the treatment is working — after you’ve renewed, after you’ve told your friends, after you stopped watching for it.
What “not established” means, and why we won’t fill it in
On long-term breast cancer risk and long-term heart risk in women taking testosterone, randomized data don’t reach far enough to say. Every page that tells you it’s proven safe long-term is claiming something nobody can support. Every page that tells you it causes cancer is doing the same thing in the other direction. The truthful answer is a shrug, and a shrug is information.It’s why the FDA panel voted the way it did in 2004.
Can testosterone cream transfer to a partner, a child, or a pet?
Yes. Topical testosterone can transfer to another person through skin-to-skin contact, which is why guidance includes handwashing after application, covering or protecting the application site, and avoiding contact that could move product onto someone else. Your pharmacy and prescriber should give you product-specific instructions, because the base, concentration, and application site all change the practical advice.
- Wash your hands immediately after applying. Every time.
- Let it dry, and follow the specific instructions for your product — drying time isn’t universal.
- Cover or protect the site as directed.
- Avoid skin-to-skin contact at the application site with anyone else — a partner, a grandchild, a kid who climbs into your lap.
- Ask what to do after accidental contact, before it happens. Ask the pharmacist.
Ask your pharmacy this specific question: “Where should I apply this, and how long until it’s safe for someone to touch that skin?”If they can’t answer it for the exact preparation they made you, that’s worth noticing.
Already taking it? Here’s what to do this week
Don’t stop or change a prescription because of a web page — including this one. Do four things instead: identify exactly what you’re on, ask your prescriber whether your total testosterone should be checked and which tests apply to you, write down every symptom with the date it started, and take all of it to your next appointment. If you have voice changes, rapid hair loss, or clitoral changes, that’s a call this week — not a note for your annual visit.
Gather these today. Ten minutes.
- A photo of every panel of the label, small print included
- The exact strength — it’ll look like “1%” or “10 mg/mL” or “5 mg/g”
- The exact amount and how often you use it
- Where you apply it, and whether you wash your hands after
- Start date, and the date of any dose change
- The pharmacy’s name and address — the one that made it, not the clinic that sold it
- Your baseline testosterone result, if there was one
- Your follow-up result, if there was one
- Every symptom, with the date it started. Write it down even if it feels silly. “Chin hair — noticed early May” is data.
Then check your plan against what should have happened
| ☐ | A clinical assessment of the actual problem — not a lab result on its own |
| ☐ | Baseline bloods before you started |
| ☐ | A recheck a few weeks in, and after any dose change |
| ☐ | Ongoing reassessment on a stated schedule |
| ☐ | Someone explained your lab's reference range, and what would trigger a review |
| ☐ | Someone asked whether you're pregnant or could become pregnant |
| ☐ | Someone asked about hair loss, acne, or unwanted facial hair before prescribing |
| ☐ | You were told what to do if you have side effects, and how quickly the route can be stopped |
Unchecked boxes aren’t proof anything is wrong. One gap is a gap. Four gaps is a pattern — and a pattern is a reason to slow down and ask.
If you already have a pellet in
First: don’t panic. A pellet isn’t a bomb. It’s a slow release you can’t adjust, which is a manageable problem once you have a number in front of you.
- Ask your prescriber whether your total testosterone should be checked now, and whether their lab offers LC-MS/MS. Ask for the actual number, not “your labs looked fine.”
- Ask what range they’re aiming for and what would trigger a review. If they can’t answer either, that’s the answer.
- Document symptoms with dates, so the conversation runs on evidence instead of vibes.
- Understand the timeline. A pellet releases for roughly three to six months. At month four you’re closer to the end than the start.
- Retrieval is a conversation to have, not a demand to make or a thing to dismiss. It’s a procedure with tradeoffs. It exists. Ask.
If you’ve had no benefit at all
Ask the question clinics don’t volunteer: has it been long enough, and is anyone going to call it? Guidance says that if there’s no meaningful improvement by around six months,testosterone should be stopped or the diagnosis reconsidered — not escalated. If the answer to “this isn’t helping” has been “let’s go up,” you’re outside the guideline, and you’re allowed to say so out loud.
How would you know if your dose is too high?
With bloods and a clinical review, not a mirror — but not by chasing a number off the internet either. ISSWSH advises against treating women to a universal target level. The goal is to keep total testosterone from significantly exceeding the upper limit of the reporting laboratory’s premenopausal reference range, interpreted alongside the assay used, the timing of the draw, your SHBG, and your symptoms. If nobody drew baseline bloods and nobody is rechecking, then nobody — including you — can tell you whether your exposure is where it should be.
Source: Parish SJ et al. ISSWSH Clinical Practice Guideline. J Sex Med. 2021;18(5):849–867.
The assay matters, and almost nobody mentions it
Most labs measure testosterone with an immunoassay. It’s fine at male concentrations. It’s less reliable at the low concentrations found in women — which is exactly the range that decides whether your exposure is where it should be. The preferred method is LC-MS/MS(liquid chromatography–tandem mass spectrometry): it measures the molecule directly rather than inferring it.
Don’t just ask for “a testosterone level.” Ask: “Is this total testosterone, and is it run by LC-MS/MS?” Ten words. Best ten words on this page.
What should be checked, and when: guideline vs. what your provider actually does
| Stage | ISSWSH guideline | Midi Health’s published policy (provider-stated, July 15, 2026) |
|---|---|---|
| Before starting | Clinical assessment; total testosterone, SHBG, fasting lipid profile, liver function | Baseline labs |
| After starting | Repeat total testosterone at 3–6 weeks | Repeat at 4–6 weeks |
| After a dose increase | Repeat within 6 weeks | — |
| Once stable | Reassess approximately every 4–6 months | Check-ins every 6–12 months (note: the ISSWSH guideline says 4–6 months once stable — a real difference) |
| No meaningful benefit by 6 months | Stop or reassess rather than escalating | — |
Read the “once stable” row again. The guideline says roughly every four to six months. The provider we link to on this page publishes six to twelve. That’s a real difference, and we’re not going to smooth it over because they’re a partner. You are allowed to ask for the guideline’s interval. That request is not rude. It’s the whole point of knowing this.
What blood work can prove — and what it can’t
A serum result reflects what ended up in your bloodstream. It does not measure what was in the tube. Absorption, timing of the draw, how you applied it, your SHBG, the assay, and your own physiology all shape that number. So a high result may reveal excessive exposure — that’s a detection system, and a good one — but it doesn’t directly tell you the finished product’s potency. Ask the question that closes the loop: “Do you do finished-product or batch-specific potency testing on this preparation, and will you give me the documentation?”A certificate for the raw ingredient is not the same as testing the cream you were handed. Monitoring isn’t optional. But it catches a problem after the product has already reached you.
Your situation has more moving parts than any article can resolve
Your form. What you’re treating. Your labs. Your history. Your state. This page can tell you what should be happening. It can’t tell you whether online care is even the right starting point for you — and for some women it isn’t. Find My HRT Path takes about 90 seconds, asks for no email, and gives you a written plan: what to verify, who to see, and a flag if your situation belongs with an in-person clinician first.
Get your personalized action plan →Is compounded testosterone safer than using a men’s product at a lower dose?
They aren’t in the same regulatory category. An FDA-approved men’s transdermal gel is an approved finished product used off-label in women — the manufacturing, labeling, and release testing were FDA-reviewed; the female use and dose were not. A compounded cream is not an approved finished product at all. The 2019 Global Consensus concluded that male formulations can be judiciously used at female doses with monitoring, and the same panel recommended against compounded testosterone.
| FDA-approved men’s gel, off-label at a female dose | Compounded cream at a female dose | |
|---|---|---|
| Finished product FDA-approved? | Yes — for men | No |
| Regulatory category of your use | Approved product, used off-label | Unapproved finished product |
| Made for your dose? | No — you measure a small fraction of a male dose | Yes — formulated at a female dose |
| Main advantage | The controls behind the number on the label | Practicality at a female dose |
| Main problem | Measuring a fraction of a male dose reliably, every day | Potency and consistency were never verified before it reached you |
| What guidelines say | Reasonable when clinically appropriate | Recommended against |
We can’t monetize the actual recommendation — and we’re making it anyway
When the guidelines say testosterone can help some women, they mean an FDA-approved product, made for men, prescribed off-label at a small fraction of the male dose, with the level checked. That’s not a loophole. That’s the actual recommendation. There is no affiliate link at the end of this paragraph and there never will be. We’re making it anyway, because leaving it out would turn everything else on this page into a sales document.
One thing to never do
Do not use your partner’s testosterone. Testosterone is a Schedule III controlled substancein the United States. Using someone else’s prescription is illegal. Beyond that: guidance commonly starts women at roughly one-tenth of a standard male transdermal dose, there is no reliable way to measure a fraction of someone else’s gel at your bathroom sink, and nobody is checking your level. Testosterone requires a prescription and a prescriber. Every time.
What to check before you fill it: the pharmacy and the six questions
Get the dispensing pharmacy’s legal name, state license, and whether it’s a 503A or 503B before you pay. Ask it to confirm its controlled-substance dispensing authority, since testosterone is Schedule III. Then ask your prescriber six questions — none of which require any medical knowledge. If a clinic can’t answer them clearly, that is the answer.
Step 1 — Get the pharmacy’s name before you pay
Not the clinic. The pharmacy— the place that physically makes the thing. You want: legal name, physical address, phone number, state license number, 503A or 503B, which state it ships from, and the exact strength of what they’re making.
Red flag
If a service won’t tell you which pharmacy is compounding your hormones until after you’ve paid, stop. That is the clearest red flag in this category, and testing for it costs you nothing.
Step 2 — Check the license yourself
Your state board of pharmacy has a lookup. Confirm: the license is active; the address matches what they told you; it’s authorized to ship into your state; no disciplinary actions. Because testosterone is a controlled substance, also ask the pharmacy to confirm its controlled-substance dispensing authority.
Step 3 — Search the public records
FDA recalls. FDA inspection observations. Warning letters. State board actions. Ten minutes, free. Finding nothing doesn’t prove quality. It proves nobody has publicly caught anything — and as we covered above, federal adverse-event reporting isn’t mandatory for 503A pharmacies.
Step 4 — Read the label like it’s a contract
Look for: your name · the drug and its exact strength · exact directions · quantity · pharmacy name · prescription number · beyond-use date · storage instructions · warnings · a pharmacist’s phone number.
That beyond-use date isn’t an expiration date. A manufactured drug’s expiration date is backed by stability testing on that product. A compounded preparation gets a beyond-use date assigned under applicable compounding standards and whatever stability information is available. Ask: “Is there product-specific stability data behind this beyond-use date for this formulation?”
Step 5 — Ask the pharmacy, and listen to the shape of the answer
| Ask this | A good answer sounds like | Worth walking away if it sounds like |
|---|---|---|
| “Are you a 503A pharmacy or a 503B outsourcing facility?” | A direct answer, plus which state licenses them | “We’re FDA registered” — that isn’t the question, and registration isn’t approval |
| “What’s the exact strength, and how do I measure a dose?” | A number and a device — a metered pump, a calibrated syringe | “A pea-sized amount” |
| “Do you do finished-product or batch-specific potency testing, and can I have the documentation?” | Either answer, stated plainly, with how often — and an offer to send it | Deflection, or “it’s bioidentical, so it’s fine” |
| “Is there stability data behind the beyond-use date for this formulation?” | A clear yes or no | A date with no basis and no interest in the question |
| “How would I find out about a recall?” | A real process — they have your contact details | Silence |
| “Can I talk to a pharmacist before I fill this?” | “Sure, hold on” | Anything else |
Step 6 — The six questions for your prescriber
- “Is this total testosterone, and is it run by LC-MS/MS?”
- “What’s my lab’s upper limit for premenopausal women, and where am I against it?”
- “When is my next blood draw?” (The guideline says a repeat total testosterone at 3–6 weeks after starting. If yours is later, ask why.)
- “If I have side effects next month, how fast can this route be stopped?” (This is the pellet question. Their answer tells you everything.)
- “Which compounding pharmacy, and do they do finished-product potency testing?”
- “Is what you’re treating me for hypoactive sexual desire disorder — or is it something else?” (If it’s something else, you’re outside the evidence, and you’re entitled to know that before you pay.)
Question six is the one that makes rooms go quiet. Ask it anyway.
If something goes wrong, here’s where it goes
- Your prescriber, first
- The dispensing pharmacist — for anything about the product itself
- Your state board of pharmacy — for dispensing or quality concerns
- FDA MedWatch — for adverse events and product-quality problems. Patients can file directly. You don’t need anyone’s permission.
Who should not start this online — and where to go instead
Some situations don’t belong in a telehealth intake. If you’re pregnant, could become pregnant, or are breastfeeding; if you have symptoms of androgen excess that haven’t been assessed; if you have a history of hormone-sensitive breast cancer; or if your symptoms haven’t been evaluated in person, this needs a clinician who can examine you — not a form.
The screening questions a careful prescriber asks
This list is drawn from the guidelines — Global Consensus 2019, ISSWSH 2021, and ACOG 2023. Use it on whoever is currently offering you testosterone.
- Signs of androgen excess — unwanted facial or body hair, hormonal acne, male-pattern hair loss
- Anti-androgen medications — such as finasteride or spironolactone
- Pregnancy, possible pregnancy, or breastfeeding
- A history of hormone-sensitive breast cancer
- What the actual diagnosis is, assessed properly — not inferred from a lab number
- Baseline bloods — total testosterone, SHBG, fasting lipids, liver function
If your main problem is painful sex, not low desire
Genitourinary syndrome of menopause is a common cause of painful sex, and it’s a tissue problem, not a desire problem. Systemic testosterone is not an established treatment for painful sex itself. Take it for that and you may conclude nothing works, when the thing that works was never tried. Look at vaginal estrogen and local optionsfirst — most of which are FDA-approved.
If your main problems are hot flashes, night sweats, or sleep
That’s standard hormone therapy territory — and unlike testosterone for women, it has FDA-approved products. Approved. Labeled. Reviewed. You’d be trading a whole category of uncertainty for nothing.
If you’re here because you’re exhausted and foggy
Someone told you testosterone was the answer. The evidence doesn’t establish that — and that’s not our opinion, it’s the Global Consensus, and it’s what the guideline’s own lead author told a hall full of menopause doctors last October. Exhaustion and brain fog in midlife have a long list of real causes: thyroid, iron, sleep apnea, depression, untreated menopause symptoms, medications, and several more worth ruling out first. You are not crazy and you are not lazy. You’re being pointed at the wrong bottle.
If any of this is urgent
Voice changes. Rapid hair loss. Clitoral changes. Bleeding that hasn’t been evaluated. New neurological symptoms. Any chance you’re pregnant.
None of that is a telehealth intake. That’s a call, this week, to someone who can examine you.
Who actually prescribes testosterone to women — and what we found when we checked
Fewer companies than the review sites suggest. Of the five major menopause telehealth platforms we checked on July 15, 2026, one — Midi Health — publishes a testosterone program for women: compounded topical cream, no pellets, in 25 jurisdictions. Everything below is what each company publishes about itself, recorded on a date. State availability changes, so confirm yours at intake rather than from any article, including this one.
| Provider | Testosterone offering? | Form | States | Monitoring (provider-stated) | Medication price | Checked |
|---|---|---|---|---|---|---|
| Midi Health | Yes | Compounded topical cream. No pellets — explicitly declined. | 25 jurisdictions: AZ, CA, CO, DC, DE, FL, IA, IL, IN, KS, MA, MD, ME, NC, NJ, NM, NV, NY, OH, OR, PA, TX, UT, VA, WA | Baseline labs → repeat at 4–6 weeks → check-ins every 6–12 months | Starts at $100 for a 90-day supply (provider-stated medication price — visits, labs, and shipping separate) | July 15, 2026 |
| Winona | No. Their own site states they do not currently prescribe testosterone. They offer DHEA. | — | — | — | — | July 15, 2026 |
| Sesame Care | No platform-wide testosterone protocol verified. It’s a marketplace; individual clinician offerings were not audited. | Varies | — | Not published at platform level | — | July 15, 2026 |
| Hers | No testosterone offering verified in current public menopause materials. | — | — | — | — | July 15, 2026 |
| Inner Balance (Oestra) | No testosterone offering found. Current public materials describe estradiol plus micronized progesterone. | — | — | — | — | July 15, 2026 |
The correction
Some third-party pages list Winona as a compounded testosterone provider. Winona’s own hormone therapy page says otherwise. Under “What types of hormones does Winona prescribe?”, their answer names estradiol, estriol, progesterone, and DHEA — and states that they do not currently prescribe testosterone. We checked on July 15, 2026.
If you’re shopping from a review site right now, that’s a live demonstration of something worth keeping: the date on a page matters more than its star rating.
Why so few platforms do this at all
Testosterone is a Schedule III controlled substance. That brings controlled-substance prescribing, dispensing, refill, recordkeeping, and state-law requirements that an estradiol patch doesn’t carry. The observable result: of the five platforms we checked, one publishes a testosterone program for women.
Here’s what we don’t like about the company we’re about to link to
Midi doesn’t offer pellets, injections, or troches.If what you want is one appointment and four months of not thinking about it, Midi will tell you no. That’s a real limitation, and for some women it’s a dealbreaker.
And that refusal is the entire reason we’re pointing you there.Because they won’t do the routes that can’t be turned off, what’s left is the route the guidelines actually endorse: topical, low dose, with published labs and a published list of who they’ll decline. They walked away from the easiest upsell in this category.
Their marketing oversells it.Midi’s own testosterone page promotes effects involving energy, mood, strength, cognition, muscle tone, and metabolic health. Those go well beyond the only consensus-recognized indication — they’re close to the exact list the Global Consensus doesn’t support and that the guideline’s lead author called out by name. We told you that five sections ago and we’re not un-telling you because they’re a partner.
And their published exclusion list is shorter than the screening list we gave you. Midi currently publishes three reasons they’ll decline: an allergy; pregnancy or breastfeeding; and active cancer treatment. That’s still shorter than the guideline-derived questions in the section above. Take our list into any consult, theirs included.
Set on a pellet anyway? Midi will decline you, and we’re not going to send you somewhere that says yes — not to a route ACOG recommends against. Go back and read the pellet evidence, then take that decision to a clinician who can examine you.
Affiliate disclosure: The link below is an affiliate link. If you start care through it, The HRT Index may earn a commission, at no extra cost to you. It didn’t change what we found — one of our partners doesn’t prescribe testosterone at all, which is why they’re not on this page. Full disclosure.
→ Check whether Midi offers testosterone cream in your state
Topical route, physiologic dose, published labs, and a provider willing to say no. Takes a minute. Eligibility, prescribing, and labs are decided during care, not by a website. Verify visit coverage with your own plan before you book. Not in a Midi state? Find My HRT Pathwill match you to what’s available where you are.
Check whether Midi Health offers testosterone in your state →Provider-stated medication price starts at $100 for a 90-day supply, checked July 15, 2026. Visits, labs, and shipping are separate. Confirm your state at intake — this page can’t do it for you.
Does “bioidentical” mean compounded testosterone is safer?
No. “Bioidentical” describes a hormone that is chemically identical to one your body produces. That’s a real chemical description — but it establishes nothing about FDA approval, manufacturing quality, correct dosing, effectiveness, or safety. There is no FDA category called “bioidentical.” ACOG notes the term is used in marketing to imply these preparations are natural and therefore safer, and that the evidence for those claims is lacking.
FDA-approved testosterone gels contain testosterone. Chemically identical to what your body makes. If “bioidentical” meant “safer,” it would apply to them too — and nobody markets an approved gel that way, because there’d be no point. The word gets deployed where there’s something else to draw attention from.
What the biggest review of this actually concluded
In 2020, the National Academies of Sciences, Engineering, and Medicine — commissioned by the FDA — published a full review of compounded bioidentical hormone therapy. Their conclusion: the evidence is insufficient to support its clinical use,and they recommended restricting it to situations where there’s a documented reason an approved product won’t work, such as an allergy or a dosage form that doesn’t exist.
NASEM. The Clinical Utility of Compounded Bioidentical Hormone Therapy: A Review of Safety, Effectiveness, and Use. 2020. doi:10.17226/25791
The NASEM carve-out, stated precisely
NASEM’s own carve-out is “a dosage form that doesn’t exist.” For testosterone in women, that’s literally the U.S. situation. It’s a much narrower argument than “it’s bioidentical” — and it’s the strongest legitimate argument for compounded testosterone that exists.
Better questions than “is it natural?”
- Was the finished product FDA-approved? (For anything compounded: no.)
- What exactly is the condition being treated?
- What route, and can it be stopped?
- How is the dose measured?
- Who made it, and what’s their record?
- How will anyone know if the exposure is too high?
Six questions. The word “bioidentical” answers none of them.
How long can a woman safely take testosterone?
Randomized trial data do not establish safety beyond 24 months. The 2019 systematic review that underpins current guidance pooled 36 randomized trials covering 8,480 women, and the longest follow-up in that body of evidence was two years. Guidance is also clear that if there’s no meaningful benefit by around six months, testosterone should be stopped or the diagnosis reconsidered — not escalated.
Two numbers do most of the work here: 8,480 women. 24 months.
“No harm found in 24 months” and “safe for 20 years” are not the same sentence
They sound similar. They’re not remotely the same claim. The first is a finding. The second is an extrapolation wearing a finding’s clothes. Any page telling you testosterone is proven safe long-term for women is doing arithmetic on data that doesn’t exist. And notice what that means for the woman starting at 52 who expects to still be on it at 70. The question isn’t “was there harm in the trials?” It’s “does anyone know what eighteen more years looks like?” The answer is no.
The six-month checkpoint
If it isn’t working by roughly six months, the guideline answer is stop or reassess. Not increase. Not add a route. Not “give it another quarter.” If your clinic’s response to “this isn’t helping” has been to raise the dose, you’ve left the evidence behind. You’re allowed to say so.
What to revisit each year
Your health history changes. Your medications change. Your menopause treatment changes. A dose that made sense at 52 may not at 60. And “we’ve been doing this for eight years” isn’t a reason — it’s a duration. Ask, every year: is this still helping, and would I start it today?
Will you still be able to get this in 2027?
Two federal threads could change access, and neither is settled. Telemedicine prescribing of controlled substances — which includes testosterone — is currently authorized through December 31, 2026 under a temporary extension, and a permanent replacement rule has not been finalized. Separately, NASEM recommended that testosterone-related substances and compounded pellet dosage forms be reviewed as candidates for a “Difficult to Compound” list; the FDA has not announced a hormone-specific final listing.
The telemedicine deadline — December 31, 2026
The flexibility that lets a clinician prescribe a controlled substance after a video visit, without an in-person exam first, currently runs through the end of this year. Without it, the Ryan Haight Act’s in-person evaluation requirement returns.
We won’t predict the outcome. A further extension or a permanent replacement rule hasn’t been finalized. If you’re on compounded testosterone through a telehealth service, this is a thing to know about, not a thing to panic about.
The “Difficult to Compound List” — and a correction
What actually happened vs. what gets reported
Several pages state that the FDA “listed” testosterone pellets on its Difficult to Compound List in 2020. That’s wrong. What actually happened: NASEM recommended that FDA’s Pharmacy Compounding Advisory Committee review ten hormones — including testosterone — plus pellet dosage forms, as candidates. A recommendation to review is not a listing. The FDA has not announced a hormone-specific final listing.
What the December 2025 FDA panel did and didn’t do
- December 10, 2025: the FDA convened an expert panel on testosterone replacement therapy for men. It looked at labeling and scheduling. It did not address testosterone for women.
- November 2025: the FDA requested removal of boxed warnings from menopausal hormone therapy. That applies to estrogen products.
Neither changed anything about testosterone for women. Any page folding these into “big FDA news for women’s testosterone” is telling you about something that isn’t there.
How The HRT Index verified this page
We sort every claim into three buckets and source them differently. Medical and regulatory facts come from the FDA, ACOG, The Menopause Society, ISSWSH, or peer-reviewed literature, named in the text. Commercial facts — who publishes what offering, in which states, at what price — come from reading providers’ own websites on a stated date, which we label “provider-stated.” Editorial conclusions are labeled as ours.
See our full The HRT Index Verification Standard.
| Item | How verified | Date |
|---|---|---|
| No FDA-approved testosterone for women in the U.S. | FDA testosterone information; Drugs@FDA | July 2026 |
| Compounded drugs are not FDA-approved | FDA, Compounding and the FDA: Questions and Answers | July 2026 |
| 503A vs. 503B obligations | FDA human drug compounding and outsourcing-facility resources | July 2026 |
| The 2004 Intrinsa advisory committee record | Contemporaneous reporting; BMJ 2004 | July 2026 |
| LibiGel safety trial completed 2012, unpublished | BC Provincial Academic Detailing evidence review, 2026 | July 2026 |
| AndroFeme approvals (Australia, NZ, South Africa, UK) | Lawley Pharmaceuticals; TGA and MHRA listings | July 2026 |
| AVA-291 January 2026 FDA Type B meeting | Company announcement (Aviva Bio) — not an FDA statement | July 2026 |
| Indication, route, monitoring, baseline testing | Global Consensus 2019; ISSWSH 2021; ACOG 2023 | July 2026 |
| Pellet hormone therapy side-effect data | Jiang X et al., Menopause 2021 | July 2026 |
| Compounded dose accuracy | Grober ED et al., J Sex Med 2015 | July 2026 |
| Voice change case series | Journal of Voice, online 2020 / print 2021 | July 2026 |
| Long-term evidence limit (36 trials, 8,480 women, 24 months) | Islam RM et al., Lancet Diabetes Endocrinol 2019 | July 2026 |
| Testosterone is Schedule III | DEA controlled substance schedules | July 2026 |
| Midi Health: 25 jurisdictions; cream; no pellets; monitoring; prices | joinmidi.com/testosterone and joinmidi.com/store/testosterone | July 15, 2026 |
| Winona: does not currently prescribe testosterone | bywinona.com hormone therapy page | July 15, 2026 |
What we didn’t verify
Whether any provider’s stated policy matches what actually happens at intake (not verified — we didn’t enrol); your specific pharmacy and prescription (not verified — we can’t); product potency, sterility, or batch quality (not independently tested by us); whether testosterone is right for you personally (this page cannot determine that). A page that tells you what it doesn’t know is the only kind worth believing about what it does.
If we got something wrong, tell us — we’ll fix it and date the fix.
Sources
- FDA — Compounding and the FDA: Questions and Answers
- FDA — Information for Outsourcing Facilities (503B duties incl. adverse-event reporting)
- FDA — Testosterone Information (approved indications are for men)
- FDA MedWatch
- DEA — Controlled Substance Schedules (testosterone = Schedule III)
- DEA — Telemedicine flexibilities in effect through Dec 31, 2026
- TGA — AndroFeme/AndroForte, Lawley Pharmaceuticals registration
- EMA — Intrinsa EPAR (2006 authorization; 2012 withdrawal)
- Davis SR et al. Global Consensus Position Statement on the Use of Testosterone Therapy for Women. J Clin Endocrinol Metab. 2019;104(10):4660–4666.
- Parish SJ et al. ISSWSH Clinical Practice Guideline for the Use of Systemic Testosterone for HSDD in Women. J Sex Med. 2021;18(5):849–867.
- ACOG. Compounded Bioidentical Menopausal Hormone Therapy. Clinical Consensus No. 6. Obstet Gynecol. 2023;142(5).
- NASEM. The Clinical Utility of Compounded Bioidentical Hormone Therapy: A Review of Safety, Effectiveness, and Use. 2020. doi:10.17226/25791
- Jiang X et al. Safety assessment of compounded non-FDA-approved hormonal therapy versus FDA-approved hormonal therapy in treating postmenopausal women. Menopause. 2021;28(8):867–874.
- Grober ED et al. Accuracy of Testosterone Concentrations in Compounded Testosterone Products. J Sex Med. 2015;12(6):1381–1388.
- Voice Change Following Testosterone Supplementation in Women: A Multi-Institutional Case Series. J Voice. Online 2020; print 2021.
- Islam RM et al. Safety and efficacy of testosterone for women: a systematic review and meta-analysis of randomised controlled trial data. Lancet Diabetes Endocrinol. 2019;7(10):754–766.
- BC Provincial Academic Detailing Service — Transdermal Testosterone for HSDD, supplement update March 2026 (records LibiGel completed 2012, unpublished).
- FDA panel rejects testosterone patch for women on safety grounds. BMJ. 2004.
- Aviva Bio — announcement of FDA guidance on AVA-291 development pathway (Jan 2026). Company-reported; not an FDA statement, not approval.
Frequently asked questions
- Is compounded testosterone FDA approved?
- No. No compounded drug is FDA-approved. The FDA does not verify a compounded drug’s safety, effectiveness, or quality before it is marketed. That is true regardless of whether the pharmacy is licensed, accredited, or well reviewed. The FDA can still inspect facilities, investigate complaints, publish recalls, and take enforcement action — what is missing is the review that happens before the product reaches you.
- Is testosterone cream safer than pellets for women?
- Topical treatment is more adjustable and more aligned with current consensus guidance than pellet therapy, and ACOG recommends preparations other than pellets for delivering testosterone to women, citing limited safety data and the inability to remove a pellet in routine practice. No head-to-head trial establishes that topical treatment is safer on every possible outcome. The clearest practical difference is that a topical can be stopped and a pellet is not designed to come out.
- Can testosterone permanently deepen a woman’s voice?
- It can. ACOG states that virilization, which includes voice deepening, may be irreversible. In short-term randomized trials using physiologic female doses there was no excess of voice change, but a case series published in the Journal of Voice described nine women whose voice changes began anywhere from immediately to four years after starting testosterone, most of them using pellets, and concluded the changes may be permanent. A case series cannot estimate how often this happens.
- How much does compounded testosterone cost for women?
- Prices vary and there is no reliable market average. As one dated data point, Midi Health currently lists its compounded testosterone cream starting at $100 for a 90-day supply, checked July 15, 2026. That is a provider-stated medication price, not a complete estimate — visits, laboratory testing, and shipping are separate. Insurance treatment varies by plan, product, pharmacy, and indication, so verify each component directly rather than relying on any published estimate.
- Why isn’t there an FDA-approved testosterone for women?
- The one submitted was rejected. On December 2, 2004, an FDA advisory committee judged the benefit of Intrinsa, a testosterone patch for postmenopausal women, clinically meaningful by a vote of 14 to 3, then voted unanimously against recommending approval because the long-term safety data were inadequate. A large safety trial called LibiGel was completed in 2012 but was never published. Australia, New Zealand, South Africa, and the United Kingdom have since authorized a 1% testosterone cream for women; the United States has approved nothing.
- Is bioidentical testosterone safer than regular testosterone?
- No. “Bioidentical” describes a hormone that is chemically identical to one the body produces. It establishes nothing about FDA approval, manufacturing quality, correct dosing, effectiveness, or safety, and there is no FDA category called bioidentical. ACOG notes the term is used in marketing to imply these preparations are natural and therefore safer, and that the evidence for those claims is lacking.
- What tests should be checked before a woman starts testosterone?
- The ISSWSH guideline calls for a clinical assessment plus baseline total testosterone, sex hormone-binding globulin, a fasting lipid profile, and liver function testing. Total testosterone should be repeated 3 to 6 weeks after starting and within 6 weeks of a dose increase, with reassessment approximately every 4 to 6 months once stable. Additional tests may be selected based on your individual history.
- Does insurance cover testosterone for women?
- Coverage varies by plan, product, pharmacy, indication, and prior-authorization rules, and the visit, the laboratory testing, and the medication may each be treated differently. Testosterone is prescribed off-label or compounded for women in the United States, both of which commonly affect coverage. Verify each component directly rather than relying on a general estimate.
- Can I use my husband’s AndroGel?
- No. Testosterone is a Schedule III controlled substance in the United States and using someone else’s prescription is illegal. Guidance commonly starts women at roughly one-tenth of a standard male transdermal dose, though the correct amount depends on the specific product and clinician instructions, and there is no reliable way to measure a fraction of someone else’s product at home. Nobody would be checking your blood level either.
- How long does testosterone take to work for low libido?
- Trials generally assessed effects over 12 weeks or longer, so it is not a fast answer. Guidance is that if there is no meaningful improvement by around six months, testosterone should be stopped or the diagnosis reconsidered rather than the dose increased.
- What testosterone level is too high for a woman?
- There is no universal number that applies across laboratories. ISSWSH advises against treating women to a single target level; the goal is to keep total testosterone from significantly exceeding the upper limit of the reporting laboratory’s premenopausal reference range. Interpretation depends on the assay used, the timing of the draw, your sex hormone-binding globulin, and your symptoms, which is why the useful question is what your own laboratory’s upper limit is and where you sit against it.
Still not sure which HRT path is right for you?
You came here asking whether compounded testosterone is safe. If you read this far, you now know the real answer depends on five things — the indication, the exposure, whether you can stop it, whether the product was ever checked, and whether anyone is monitoring you. No article can resolve those for your situation. That’s what the tool is for. Take our free 90-second matching quiz.No email. You’ll get a written plan: what to verify before your consult, which providers fit your state and situation, and a flag if your situation belongs with an in-person clinician first.
Find My HRT Path →Educational content only. Not medical advice, and not reviewed by a clinician. Do not start, stop, or change a prescription based on this page. Talk to your prescriber or your pharmacist.