What we actually verified for this page ()
We read the FDA prescribing label, The Menopause Society's 2023 nonhormone guidance, the randomized human trials, and the current public pages for each provider (treatment language, pricing, insurance, and drug lists). We reviewed publicly displayed coupon and cash-price examples — final prices vary by dose, quantity, pharmacy, ZIP code, and insurance. We did not sit through an intake or consult, so we can't promise any single clinician will prescribe oxybutynin to any single person.
Does oxybutynin actually work for hot flashes?
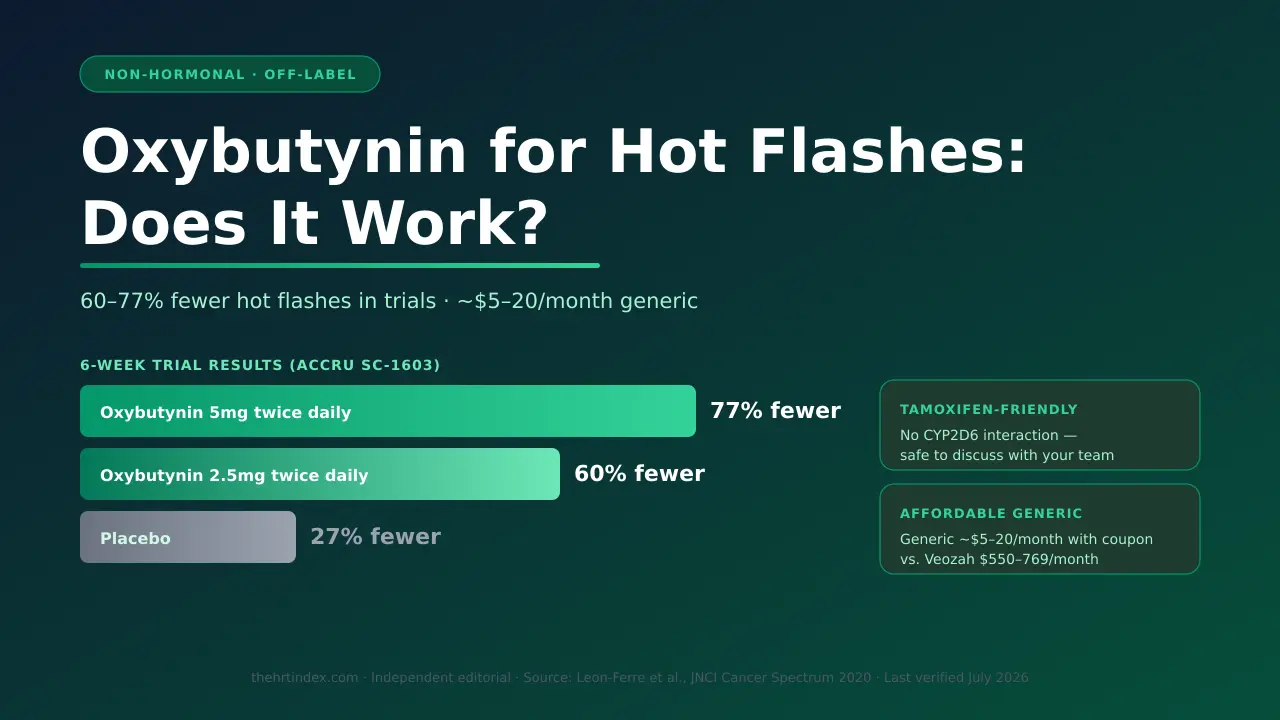
Yes. In a six-week randomized trial of 150 women, oxybutynin lowered how often hot flashes happened by 60–77%, versus 27% on placebo — and a combined frequency-and-severity score dropped 70–86%. It's one of the better-evidenced non-hormone options, though the studies were short and long-term results aren't settled.
Here's the part that trips people up: oxybutynin is a bladder drug. So why would it touch a hot flash? Oxybutynin blocks a body-signaling chemical called acetylcholine — that's what makes it an "anticholinergic." Doctors first used it to calm an overactive bladder. Along the way, they noticed people on it sweated less. Researchers suspected that reduced-sweating effect might help hot flashes and tested it. It did — though the exact reason it works for hot flashes hasn't been fully pinned down.
The clearest proof comes from a study led by Mayo Clinic's Dr. Roberto Leon-Ferre, published in JNCI Cancer Spectrum in 2020 (the "ACCRU SC-1603" trial). 150 women, each having at least 28 hot flashes a week. Average age 57. Two-thirds (65%) were on tamoxifen or an aromatase inhibitor — women who usually can't take estrogen.
Trial results by group — sourced from Leon-Ferre et al., JNCI Cancer Spectrum, 2020 (ACCRU SC-1603 / NCT02961790).
| Group | Hot flashes cut per day | How much less often | Frequency + severity score |
|---|---|---|---|
| Oxybutynin 5 mg twice daily | 7.5 fewer | 77% fewer | 86% lower |
| Oxybutynin 2.5 mg twice daily | 4.8 fewer | 60% fewer | 70% lower |
| Placebo (sugar pill) | 2.6 fewer | 27% fewer | 29% lower |
So when you see "up to 86%," that's the combined score (how often plus how badly), not the frequency alone. The honest headline is: hot flashes happened 60–77% less often. Still strong for a non-hormone pill — but now you know exactly what the number means.
A couple of other studies back this up. A 12-week trial of a once-daily extended-release version (Simon et al., Menopause, 2016) also beat placebo. And a retrospective chart review of 52 cancer patients — more than 90% of whom had hot flashes that hadn't responded to earlier treatments — found about 70% got a partial or strong response (Sexton et al., Menopause, 2007). That last one wasn't a randomized study, so treat it as supportive context.
The honest counterweight: these trials ran only six to twelve weeks, in specific groups of women, and they don't tell us what happens after years of use. Think of oxybutynin as a strong option to try, not a guarantee.
The Menopause Society's 2023 Nonhormone Therapy Position Statement lists oxybutynin as a recommended non-hormone option for hot flashes, at "Level I–II" evidence. It's not as effective as hormone therapy — which remains the most effective treatment overall — but for women who can't or won't use estrogen, it earns its place. → Compare all non-hormonal options
Is oxybutynin FDA-approved for hot flashes? The off-label truth
No. Oxybutynin is FDA-approved for overactive bladder — not hot flashes. Using it for hot flashes is "off-label." That's legal and common, and it's backed by real trials and menopause-society guidance, but it means the FDA hasn't formally reviewed it as safe and effective for this exact use.
Off-label prescribing is when a clinician uses an approved drug for a condition that isn't on its official label. It happens every day, across all of medicine, and it's completely legal. The FDA itself says clinicians may prescribe an approved drug for an unapproved use based on their judgment.
| This IS true | This is NOT true |
|---|---|
| Oxybutynin is an FDA-approved drug. | Oxybutynin is FDA-approved for hot flashes. (It's not.) |
| A clinician can legally prescribe it off-label for hot flashes. | Off-label means experimental, shady, or illegal. |
| Trials and The Menopause Society support this use. | It's been proven better than the drugs the FDA did approve for hot flashes. |
One clarification: oxybutynin is a standard, FDA-approved generic being used off-label. It is not a compounded drug. Those are different things, and we never blur them. Clinicians reach for it when a woman can't take estrogen, has already tried something that didn't work, or wants a cheaper, non-hormone option.
The honest downside: side effects, the dementia question, and heat
Oxybutynin's most common side effects are dry mouth and constipation. Its biggest real concern is that it's an anticholinergic — a drug class linked in long-term studies to a higher risk of memory problems and dementia, mostly with prolonged use in older adults. It also lowers sweating, which can make dangerous overheating a real risk in hot weather or hard exercise.
The everyday side effects. Most are mild, and they line up with what any "drying" drug does:
- Dry mouth — the most common, by far.
- Constipation.
- Dry eyes, blurred vision.
- Dizziness or drowsiness.
- Trouble starting to pee (ironic for a bladder drug, but real).
- Less sweating (the effect that helps hot flashes — but see the heat warning below).
- At higher doses, some women reported mild confusion.
Does oxybutynin cause dementia?
This is the question that drives the scary headlines, so here's the honest version. Anticholinergic drugs can cross into the brain, and large observational studies link long-term, cumulative anticholinergic use to a higher risk of dementia — especially in older adults. One long-term study linked taking oxybutynin at 5 mg a day for more than three years to greater dementia risk. The 2023 American Geriatrics Society Beers Criteria flags oxybutynin for caution in people 65+.
Read the nuance carefully: These studies show an association, not proof that oxybutynin caused dementia in any one person. The strongest signals came from older adults taking it at higher doses for years. The hot-flash trials ran only six to twelve weeks. Bring your full medication list (including allergy pills, sleep aids, and older antidepressants) to whoever you see, and ask them to look at your total anticholinergic load.
The heat warning people forget
Oxybutynin works partly by lowering sweating — and sweating is how your body cools itself. The FDA label specifically warns about heat prostration (dangerous overheating) in high temperatures. If you work outdoors, do hard cardio, love hot yoga, or spend summers somewhere brutal, that's a real conversation to have with your clinician.
Hard "no" situations (from the FDA label)
- Urinary retention (trouble emptying your bladder).
- Gastric retention or severe slow-gut (decreased gastrointestinal motility) condition.
- Uncontrolled narrow-angle glaucoma.
Sources: FDA/DailyMed oxybutynin prescribing information; AGS 2023 Beers Criteria; SUFU overactive-bladder cognitive-safety white paper; Cleveland Clinic Journal of Medicine, 2024.
Oxybutynin is NOT the right first move if you're 65 or older, or already on several drying medicines. If that's you, the anticholinergic load matters more, and a bladder-selective option or the FDA-approved hot-flash drug Veozah may be the better conversation. But because the hot-flash doses studied are low, and because oxybutynin doesn't interfere with tamoxifen the way some antidepressants do, for many women who can't take estrogen it's one of the smartest, cheapest options to ask about. See the two ways to get it prescribed online → · Compare lower-risk options with Find My HRT Path →
Who oxybutynin is right for — and who should take extra care
Oxybutynin fits best for women who can't take estrogen, especially those on tamoxifen or those who also have bladder urgency. It calls for extra caution — not an automatic no — in women 65 and older or on other anticholinergic drugs, and it's the wrong tool for uncontrolled narrow-angle glaucoma, bladder-emptying problems, or vaginal dryness.
🟢 GREEN LIGHT — worth asking about
- You can't (or won't) take estrogen and want a non-hormone option
- You're on tamoxifen — oxybutynin's sweet spot
- You also have urinary urgency or overactive bladder
- You tried antidepressants for hot flashes and hated the side effects
🟡 YELLOW LIGHT — ask, but weigh it
- You're 65 or older, or take other "drying" medicines — brain-load concern is higher
- You have frequent constipation or dry-eye issues already
- You run hot for work or exercise (the sweating/heat issue)
🔴 RED LIGHT — probably not your medicine
- Uncontrolled narrow-angle glaucoma, trouble emptying your bladder, or a severe slow-gut condition — label "do not use" flags
- Your main problem is vaginal dryness or painful sex → local vaginal estrogen is what helps that
- You only want a drug the FDA approved for hot flashes
Want your situation matched before you book anything? Build my safest starting route with Find My HRT Path →
Why women on tamoxifen keep choosing oxybutynin
Oxybutynin avoids the specific drug-interaction problem that paroxetine (Brisdelle) has with tamoxifen. It's cleared by a liver enzyme called CYP3A4 and doesn't block CYP2D6 — the enzyme tamoxifen needs to work. The big trial also included many women on tamoxifen. That doesn't prove blanket safety, but it's a real edge, and it's why oxybutynin is worth raising with your care team.
Tamoxifen is a common breast cancer medicine. Your body has to activate it using a liver enzyme called CYP2D6 (think of CYP2D6 as a key that switches tamoxifen "on"). Some hot-flash drugs — especially paroxetine (Brisdelle) — jam that key. Brisdelle's own FDA label says paroxetine lowers the level of an active tamoxifen metabolite and recommends considering avoiding the combination. That's not a small deal.
Oxybutynin doesn't touch that key. It's broken down by a different enzyme (CYP3A4) and doesn't block CYP2D6, so it doesn't create that same interaction. That's exactly why the big oxybutynin trial was built around breast cancer patients — two-thirds were on tamoxifen or a similar drug, and it worked.
One honest boundary: that trial didn't measure cancer recurrence or long-term outcomes, so "avoids the paroxetine interaction" isn't the same as "proven 100% safe with your cancer treatment." The final call still depends on your age, other medicines, and coordination with your oncology team. If you're a survivor who's been told "no hormones" and antidepressants clashed with your cancer meds — this is the option worth raising, with your oncology and prescribing teams in the loop.
Sources: Breastcancer.org; Brisdelle (paroxetine) FDA label; Mayo Clinic ACCRU trial protocol (CYP3A4 metabolism, no CYP2D6 inhibition).
Is oxybutynin a better fit if you also have an overactive bladder?
Possibly. Oxybutynin is FDA-approved for overactive bladder and separately has good short-term evidence for hot flashes — so if you have both, it's a rational medicine to discuss. No trial has proven it treats both at once in the same women, so treat this as a reason to raise it, not a guaranteed two-for-one.
Menopause and bladder trouble love to show up together. Oxybutynin is one of the few options that lands on both. Its approved job is calming an overactive bladder; its off-label bonus is calming hot flashes. If both are wrecking your sleep, it's a reasonable single medicine to bring up.
Two honest caveats:
- New or unusual bladder symptoms (pain, blood, burning, repeated infections, trouble emptying) need a proper look first — don't assume it's "just menopause."
- If your bladder issue is really vaginal/urinary dryness (a burning, thinning feeling, or painful sex), that's a different problem called GSM. Oxybutynin does nothing for that — local vaginal estrogen and similar treatments are what actually help.
Oxybutynin vs. the other non-hormonal options for hot flashes
Oxybutynin is one of the cheapest options and sidesteps the tamoxifen interaction, but it's off-label with the anticholinergic concern. Veozah and Lynkuet are FDA-approved for hot flashes but pricey and require liver monitoring. Brisdelle is FDA-approved but can interact with tamoxifen. The best pick depends on your budget, other health issues, and whether you're on tamoxifen.
Important: effectiveness figures come from different trials with different designs and endpoints — read them as rough guides, not a head-to-head race. Prices are U.S. cash estimates checked and vary by dose, quantity, pharmacy, and location.
| Option | FDA-approved for hot flashes? | How well it works (separate trials) | Cash cost/month | Tamoxifen (CYP2D6)? | Key catch / monitoring |
|---|---|---|---|---|---|
| Oxybutynin (generic) | No — approved for bladder; off-label for hot flashes | ~60–77% fewer hot flashes (6-week trial) | ~$5–20 with coupon | No CYP2D6 conflict | Anticholinergic; dry mouth; lowers sweating; long-term dementia caution; no lab monitoring |
| Fezolinetant (Veozah) | Yes (May 2023) | ~60% fewer at 12 weeks | ~$550–769 cash | No | Boxed warning for liver injury; requires liver tests before, monthly ×3, then months 6 & 9 |
| Elinzanetant (Lynkuet) | Yes (Oct 2025) | Significant reduction in trials; may also help sleep | Brand — price not yet verified | No | Requires baseline and 3-month liver tests; check current label |
| Paroxetine (Brisdelle) | Yes (2013) | Mild–moderate | Brand ~$200–400; generic ~$15–40 | ⚠️ Can interact — consider avoiding with tamoxifen | SSRI side effects; usually avoided in tamoxifen users |
| Venlafaxine (Effexor XR) | No (off-label) | ~30–50% fewer | Generic ~$10–30 | Fewer CYP2D6 concerns than paroxetine | Can raise blood pressure; taper to stop |
| Gabapentin | No (off-label) | Modest; useful for night sweats/sleep | Generic ~$10–30 | No | Drowsiness, dizziness; often dosed at night |
| Clonidine | No (off-label) | Weakest of this group (~26–38%) | Generic ~$10–30 | No | Blood-pressure drug; not first-line; rebound spikes if stopped fast |
Sources: FDA/DailyMed and drug labels; The Menopause Society 2023; Cleveland Clinic Journal of Medicine 2024; GoodRx, SingleCare & Drugs.com (July 2026). Also see: Veozah vs. Lynkuet full comparison →
How to read the table for your life:
- Lowest cost and no tamoxifen clash? → Oxybutynin.
- Want an FDA-approved-for-hot-flashes drug and can handle monitoring/cost? → Veozah or Lynkuet.
- Night sweats and broken sleep are the real problem? → Ask about gabapentin.
- On tamoxifen? → Paroxetine is usually avoided; oxybutynin or venlafaxine make more sense.
Not sure which of these is your match? Compare them against your exact situation → Find My HRT Path
Oxybutynin dosage for hot flashes: what the studies used
The trials studied plain (immediate-release) oxybutynin at 2.5–5 mg twice a day, over six to twelve weeks. Those are study regimens, not a personal prescription — your dose, schedule, and when to reassess are decisions for your clinician. Onset varies from woman to woman, and long-term use hasn't been studied.
- What the studies used: immediate-release oxybutynin at 2.5 mg or 5 mg, twice daily. There's also an extended-release once-a-day version, but the hot-flash study used a higher 15 mg dose that caused more dry mouth — lower doses are generally preferred.
- Timeline: trials measured results at six and twelve weeks. Some patient guidance notes women may notice a change within a couple of weeks, but there's no single guaranteed onset.
The firm boundary: those are study doses, not your prescription. The right dose and schedule depend on your age, other medicines, kidneys, liver, and how you tolerate it. Don't self-adjust, and don't start or stop it on your own. One genuinely handy fact: unlike clonidine or venlafaxine, oxybutynin doesn't require a slow taper — but any change should still go through your prescriber.
What medicines interact with oxybutynin?
Oxybutynin's biggest interaction risk is stacking with other "drying" (anticholinergic) medicines. Strong CYP3A4-blocking drugs can raise its levels, it can slow the absorption of other medicines, and mixing it with alcohol or sedatives can worsen drowsiness. Give your clinician your full medication, over-the-counter, and supplement list.
- Other anticholinergic medicines. Some allergy pills (like diphenhydramine/Benadryl), sleep aids, older antidepressants, bladder medicines, and motion-sickness drugs are also "drying." Combining them increases dry mouth, constipation, confusion, and the cumulative brain-load concern.
- Strong CYP3A4 inhibitors. Certain antifungals and some antibiotics can raise oxybutynin levels in your body, which can mean more side effects.
- Slowed gut movement. Because oxybutynin can slow the gut, it may change how well other medicines are absorbed.
- Prokinetics like metoclopramide. Oxybutynin can work against medicines meant to speed up the gut.
- Alcohol and sedatives. These can add to drowsiness and dizziness.
None of this makes oxybutynin unusable — it means the clinician needs your complete list to check for overlap. (Source: FDA/DailyMed oxybutynin label.)
When should you get urgent medical help while taking oxybutynin?
Seek urgent care if you experience:
- You can't pee (possible acute urinary retention).
- Severe confusion, hallucinations, or marked agitation.
- Signs of heat stroke — hot, dry skin, confusion, feeling faint in the heat (oxybutynin lowers your ability to sweat and cool down).
- Swelling of the face, lips, tongue, or throat, or trouble breathing (possible allergic reaction/angioedema).
- Sudden severe eye pain or a sudden change in vision.
If any of these happen, don't wait for a telehealth follow-up — get in-person emergency care. (Source: FDA/DailyMed oxybutynin label.)
What oxybutynin for hot flashes really costs
The medicine itself is usually cheap — generic oxybutynin often runs just a few dollars to around $20 a month with a pharmacy coupon. The bigger cost is the telehealth visit, which ranges from about $34 for a single cash-pay visit to $250 for a first visit with a menopause specialist.
"How much does oxybutynin cost?" has two answers, and mixing them up is how people get surprised. Here they are separately.
Bucket 1: the drug itself (usually cheap)
Prices checked — confirm at your pharmacy, as they vary by dose, quantity, and location.
- Generic immediate-release: as low as about ~$19.99 with a GoodRx coupon; as low as ~$4.81 with a SingleCare coupon for 30 tablets
- Generic extended-release (Ditropan XL): as low as about ~$6.60 with a GoodRx coupon
- Brand-name Ditropan XL: much higher, roughly $228–260
Two quick notes: coupon prices change by pharmacy and ZIP code. A "30-tablet" price isn't a full month if you take it twice a day (that's 60 tablets). Even so, for most women the generic lands somewhere between pocket change and about $20 a month. For perspective: Veozah runs $550–769 cash. Oxybutynin is one of the cheapest paths to relief there is.
Bucket 2: the visit (your real cost)
Provider visit costs — sourced from Sesame and Midi Health pricing pages.
| Route | Visit cost | Notes |
|---|---|---|
| Sesame (cash-pay) | Visits as low as $34 | No insurance needed; drug billed separately at your pharmacy |
| Midi Health (uses insurance) | $250 first / $150 follow-up self-pay (~$50 with insurance) | Midi says most insured patients pay around $50 out of pocket; exact cost depends on your plan |
Smart insurance questions to ask (off-label can be covered — just confirm):
- Is oxybutynin covered on my plan, and at what copay?
- Does it need prior authorization?
- Is immediate-release or extended-release preferred?
- Is this telehealth clinician in-network?
Want to see which route fits your budget and insurance? Match my situation with Find My HRT Path →
How to get oxybutynin for hot flashes online
You can get oxybutynin prescribed by telehealth because it's not a controlled substance — so no special federal in-person rule applies. A video visit works in most cases, as long as the clinician is licensed in your state and decides it's appropriate. The two practical routes are a menopause specialist who takes insurance (Midi Health), or a fast, low-cost cash-pay visit (Sesame).
Provider comparison — sourced from public provider pages.
| Provider | Menopause-focused? | Names oxybutynin for hot flashes? | Visit price | Insurance? | Prescription guaranteed? |
|---|---|---|---|---|---|
| Midi Health | Yes | Yes — names it among non-hormonal hot-flash options | $250 first / $150 follow-up self-pay (~$50 with insurance) | In-network most PPO plans; no Medicare/Medicaid | No |
| Sesame | General marketplace (has menopause option) | No — its oxybutynin page covers only overactive bladder | Visits from $34 | Cash-pay only | No |
Route 1 — Midi Health
Best if you want insurance and a menopause specialist
Midi is a menopause-focused telehealth service that publicly names oxybutynin as one of the non-hormonal options for hot flashes — more than most telehealth services do. It offers the full non-hormonal toolkit alongside HRT, it's in-network with most PPO plans, it operates in all 50 states, and you get a live video visit with a prescriber — not just a questionnaire.
- Cost: $250 first visit, $150 follow-up if you self-pay; Midi says most insured patients pay around $50 out of pocket per visit (the visit fee doesn't include the medication).
- Insurance limits: Midi cannot treat Medicaid or Medi-Cal patients (even as self-pay), and it's not covered by Medicare.
- Realistic expectation: whether oxybutynin specifically is the right pick is a decision made at your visit. Go in ready to discuss it.
Best for: overlapping symptoms, insurance users, and anyone who wants one clinician who knows her whole story — especially breast cancer survivors navigating "no hormones." → Read our full Midi Health review
Check Midi's coverage in your state →Route 2 — Sesame
Best if you're cash-pay or want the lowest visit price
Sesame is a direct-pay telehealth marketplace: visits start as low as $34, no insurance needed, in all 50 states. Because oxybutynin isn't a controlled substance, a clinician can prescribe it if it's appropriate.
Honest catch we verified: Sesame's dedicated oxybutynin page is written entirely for overactive bladder — it doesn't mention hot flashes, and oxybutynin isn't listed in Sesame's visible menopause treatment options. That doesn't mean a Sesame clinician won't discuss it for hot flashes — but confirm the clinician will evaluate off-label oxybutynin for hot flashes before you pay.
Best for: uninsured or high-deductible women who want the lowest visit price and are comfortable confirming the off-label use with the clinician up front. → Read our full Sesame review
See Sesame's clinicians and current prices →Red flags on any "get it online" site — walk away if you see:
- "Guaranteed" prescription. No honest clinician promises that.
- No named, licensed clinician or state-licensure info.
- No questions about your other medicines or your glaucoma/bladder history.
- No mention that hot-flash use is off-label.
- A countdown timer or a fake "shortage."
What about the over-the-counter Oxytrol patch?
Don't swap the studied oral oxybutynin for the over-the-counter Oxytrol for Women patch. The OTC patch is approved for overactive bladder, not hot flashes, and the evidence from the oral hot-flash trials can't be transferred to the patch.
The hot-flash studies used oral oxybutynin at specific doses, tracked by researchers. The OTC patch (Oxytrol for Women) was approved for bladder symptoms, delivers the drug differently, and hasn't been studied the same way for hot flashes. Buying a bladder patch and hoping it doubles as hot-flash treatment isn't a plan — it's a guess. If you want to try oxybutynin for hot flashes, do it through a clinician who can match the form and dose to you.
What did the trials show about sleep and daily life?
Beyond fewer hot flashes, the six-week ACCRU trial found that women on the effective dose reported measurable improvements in sleep, mood, and social and leisure activities. That's documented outcome data, not marketing.
In the ACCRU trial, women didn't just report fewer hot flashes — those on the effective dose reported real improvements in sleep, mood, and social and leisure life. That's published trial data. The trial's lead, Dr. Roberto Leon-Ferre of Mayo Clinic, has described a practical way clinicians think about it: oxybutynin can help most during the worst stretch of hot flashes, with the hope of easing off later as symptoms settle.
Note on reviews: any patient stories you see on a provider's own website are care-experience testimonials the company chose to publish. They can be reassuring, but they're not independent evidence that a drug works or is safe for you. Individual results vary; the only way to know if it's your answer is to try it under proper guidance.
Frequently asked questions
Is oxybutynin a hormone?
No. It's an anticholinergic (antimuscarinic) medicine, FDA-approved for overactive bladder. It contains no hormones, so it's an option for women who can't or don't want to take estrogen.
Is oxybutynin FDA-approved for hot flashes?
No. It's FDA-approved for overactive bladder. Using it for hot flashes is off-label — legal and supported by trials and The Menopause Society's 2023 guidance, but not formally FDA-reviewed for that use.
Does oxybutynin really help hot flashes?
Yes. In a six-week randomized trial, hot flashes happened 60–77% less often on oxybutynin, versus 27% on placebo. A combined frequency-and-severity score fell 70–86%. It's not as strong as hormone therapy, but it's one of the better-evidenced non-hormone options.
Can an online doctor prescribe oxybutynin for hot flashes?
Yes. It's not a controlled substance, so a licensed telehealth clinician can prescribe it after a video visit, as long as they're licensed in your state and decide it's appropriate. A prescription is never guaranteed.
What dose of oxybutynin was studied for hot flashes?
Trials used immediate-release oxybutynin at 2.5 mg or 5 mg twice daily, over six to twelve weeks. Those are study regimens, not personal instructions — your clinician sets the right dose for you.
How long does oxybutynin take to work?
The trials measured results at six and twelve weeks. Some patient guidance mentions a change within a couple of weeks, but there's no single guaranteed onset time — your prescriber decides when to reassess.
Can I take oxybutynin with tamoxifen?
Oxybutynin avoids the specific interaction that paroxetine has with tamoxifen — it doesn't block CYP2D6, the enzyme tamoxifen needs to work — and the main trial included many tamoxifen users. That doesn't prove full safety with your cancer treatment, so review it with your oncology and prescribing teams.
Does oxybutynin cause dementia?
It's an anticholinergic, a class linked in long-term studies to higher dementia risk, mostly with prolonged higher-dose use in older adults. These studies show association, not proof of cause, and the hot-flash trials were short. Review your total anticholinergic load with a clinician, especially if you're 65 or older.
What are oxybutynin's side effects?
Most commonly dry mouth and constipation, plus possible dry eyes, dizziness, and mild confusion at higher doses. It also lowers sweating, which can risk dangerous overheating in heat or hard exercise. Not used with uncontrolled narrow-angle glaucoma, urinary retention, or severe slow-gut conditions.
What medicines interact with oxybutynin?
Mainly other 'drying' (anticholinergic) medicines, which add up the side effects. Strong CYP3A4-blocking drugs can raise its levels, and alcohol or sedatives can worsen drowsiness. Share your full medication and supplement list with the clinician.
Can I use the over-the-counter Oxytrol patch for hot flashes?
Don't assume so. The OTC Oxytrol patch is approved for bladder symptoms, and the hot-flash evidence is for oral oxybutynin under clinical care. The evidence doesn't transfer from the pills to the patch.
Is oxybutynin safe after age 65?
Age 65 isn't an automatic no, but it makes the cognitive and anticholinergic-load review more important — the Beers Criteria flags oxybutynin for caution in older adults. It's a careful conversation, and sometimes another option fits better.
How much does oxybutynin cost without insurance?
Often just a few dollars to around $20 a month generic with a pharmacy coupon; prices vary by dose, quantity, pharmacy, and location. The bigger cost is usually the visit — from about $34 for a cash-pay telehealth visit. Prices as of July 2026 — confirm at your pharmacy.
Oxybutynin vs. Veozah — which is better?
Veozah is FDA-approved for hot flashes and targeted, but costs roughly $550–769 per month cash and carries a boxed liver-injury warning with required liver testing. Oxybutynin is far cheaper and sidesteps the tamoxifen interaction, but it's off-label with an anticholinergic caution. The right choice depends on cost, coverage, and your health history.
Still deciding?
Oxybutynin is a legitimate, affordable, non-hormonal option. For the right woman — especially one on tamoxifen or dealing with bladder urgency too — it can be genuine relief. It's not for everyone, and we'd rather you land on the right answer than any answer.
Take Find My HRT Path — free, 90 seconds →Sources
Medical and regulatory (primary): U.S. FDA / DailyMed — oxybutynin prescribing information (indications, contraindications, warnings, interactions; DEA schedule: none); FDA Veozah (fezolinetant) label and liver-injury safety communication; FDA Lynkuet (elinzanetant) label; FDA Brisdelle (paroxetine) label.
Clinical guidance and peer-reviewed research: The Menopause Society, 2023 Nonhormone Therapy Position Statement (Menopause, 2023); Leon-Ferre et al., JNCI Cancer Spectrum, 2020 (ACCRU SC-1603 / NCT02961790); Simon et al., Menopause, 2016; Sexton et al., Menopause, 2007; Cleveland Clinic Journal of Medicine, 2024; American Geriatrics Society 2023 Beers Criteria; SUFU overactive-bladder cognitive-safety white paper; Breastcancer.org (tamoxifen interaction).
Provider-stated commercial information: Midi Health (treatment content, pricing, insurance pages), July 2026; Sesame (oxybutynin and menopause pages, pricing), July 2026.
Dated pharmacy/coupon examples: GoodRx, SingleCare, Drugs.com — Prices vary by dose, quantity, pharmacy, and location — confirm at checkout.
See our methodology and editorial team for how we verify and maintain this content.