This page is for you if:
- You’ve got a patch-shaped red or itchy mark
- Welts that keep coming back after each patch
- Irritation that lingers after you peel the patch off
- A rash that started after a pharmacy refill
- You’re wondering whether a different patch would be gentler
This page can’t handle:
- Trouble breathing or swallowing — call 911
- Face or throat swelling — call 911
- Fast-spreading rash — same-day care
- Signs of infection
- The decision to stop or change your prescription
What we actually verified —
We reviewed the current product labeling on DailyMed for every estradiol patch in our comparison table — patch size at each dose, adhesives, other listed ingredients, and application instructions. We cross-checked marketing status with manufacturers and reviewed MedlinePlus and dermatology guidance for skin-reaction and emergency signs. Last verified: using The HRT Index Verification Standard.
We did not wear these patches and cannot diagnose your rash. Trial percentages are label evidence — not a prediction of what will happen to you.
What should I do right now about an estradiol patch rash?
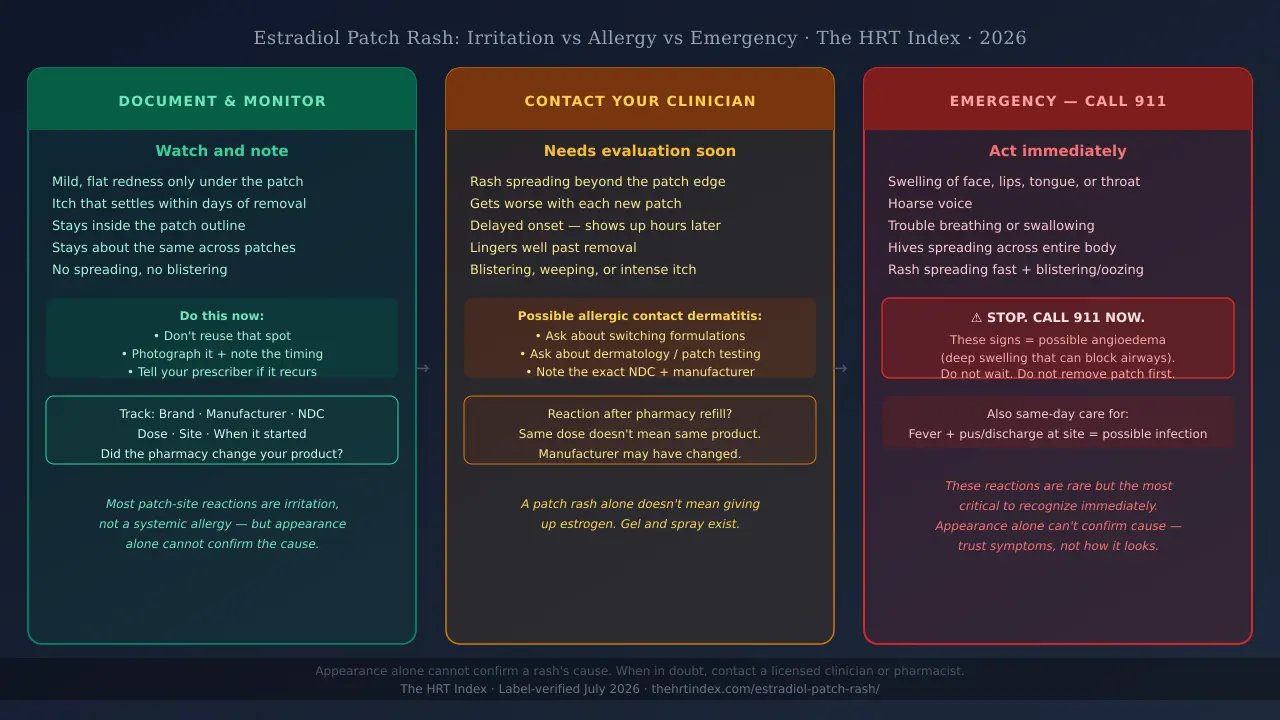
First, rule out an emergency: face or throat swelling, a hoarse voice, or trouble breathing or swallowing means call 911. A rash that’s spreading fast, blistering, oozing, or covering your body means same-day medical care. If it’s a mild mark limited to the patch area and you otherwise feel fine, don’t reuse that spot — photograph it, note the timing, and tell your prescriber or pharmacist if it keeps happening.
Think of it as three levels: emergency, get-seen-soon, and document-and-monitor. The guide below sorts what you’re seeing into the right level. It can’t tell you why your skin reacted — no chart can do that from a description — but it can tell you how fast to act.
The estradiol patch rash decision guide
| What you’re seeing | What it might mean (not a diagnosis) | What to do |
|---|---|---|
| Swelling of the face, lips, tongue, or throat; hoarse voice; trouble breathing or swallowing | Possible serious allergic reaction (angioedema) | ⚠ Call 911 or go to the ER now. Don’t stop to troubleshoot the patch online. |
| Hives spreading across your body, or a rash spreading fast beyond the patch; blisters that ooze or weep | Possible severe contact dermatitis, wider reaction, infection, or another skin condition | Get same-day medical help. If hives come with facial/throat swelling or trouble breathing, call 911. |
| Growing pain, pus or discharge, warmth, fever, chills, or feeling generally unwell | Possible skin infection | Get urgent medical advice. |
| Intensely itchy, raised welt at the patch site that gets worse with each new patch and lingers after removal | Possible allergic contact dermatitis (immune reaction to something in the patch) | Contact your clinician soon. Ask about switching formulations or a dermatology referral for patch testing. |
| Mild, flat redness or itch, only under the patch, that settles within a few days after removal | Possible ordinary application-site irritation | Don’t put the next patch on that spot. Photograph it, note when it started, and tell your prescriber or pharmacist if it’s recurrent or bothersome. |
| A reaction that suddenly shows up after months of no trouble | Possible new sensitivity — or a changed product | Document each one and ask whether your pharmacy switched manufacturers. |
Patch Rash Check — Coming Soon
Our free Patch Rash Check tool will let you answer a few questions about what your skin is doing and build a short, copy-ready message you can hand or send to your doctor or pharmacist — with warning signs flagged. While it’s in development, use Find My HRT Path to match your situation to the right care route.
Find My HRT Path → (free, ~90 seconds)Is an estradiol patch rash normal — or could it be an allergy?
A mild red or itchy mark under an estradiol patch is a recognized, common side effect — but “common” doesn’t mean every rash is harmless, and appearance alone can’t tell you whether it’s plain irritation or a true allergy. Reported rates vary widely depending on the product and study, but application-site reactions appear in roughly 10% to 25% of users — and most of those are irritation rather than a true allergy.
Patterns that raise concern — not a home diagnosis
| Often more reassuring | Should raise more concern | |
|---|---|---|
| Where it is | Stays inside the patch outline | Spreads clearly beyond the patch edges |
| When it starts | Soon after applying | Delayed — showing up a day or more later |
| Over repeated patches | Stays about the same, or settles | Gets worse with each new patch |
| After removal | Eases within a few days | Lingers well beyond removal |
The honest catch:these are hints, not a verdict. Both kinds of contact dermatitis can look very similar — intense itch, redness, swelling, even blisters or weeping can happen with either — and appearance alone can’t identify which you have or which ingredient is behind it (American Academy of Dermatology). The emergency signs above override everything.
One thing most pages miss: it can look different on darker skin
Most rash advice assumes redness. On brown or Black skin, irritated or inflamed skin may not look red — it can look darker brown, purple, or gray, or show up mainly as swelling, warmth, or a change in texture. Don’t wait for “redness” to decide something’s wrong. Trust itch, swelling, raised skin, blistering, and how the area feels.
Why is the patch causing a rash — the glue or the estrogen?
Both irritant and allergic reactions are possible, and the culprit can be the adhesive, another inactive ingredient, the simple fact of skin being sealed under a patch, friction — or, rarely reported in case studies, estradiol itself. The reassuring part:because it’s usually not the hormone, the fix is often a change of patch or delivery method rather than giving up estrogen.
A patch is more than hormone. A typical estradiol patch has a backing film, an adhesive layer (containing the drug plus other ingredients that help it cross the skin), and a liner you peel off. A few ingredients on these labels are worth knowing:
Propylene glycol
A very common ingredient in skincare and medicines, and a recognized cause of contact allergy in some people. In a 2021 case report (JAAD Case Reports), propylene glycol in an estradiol patch was identified as the cause of one woman's allergic reaction — not the estrogen. A case report shows what's possible in one patient; it doesn't tell you how often it happens or what caused your rash.
Oleyl alcohol
A fatty alcohol used to help absorption — another ingredient that can irritate some skin.
Acrylic/acrylate adhesives
The sticky base used in every patch in our comparison table. Some people can react to the adhesive itself, independent of any other ingredient.
Because different patches contain different ingredients and cover different amounts of skin, the specific patch you use isn’t a trivial detail — it’s a lever you and your prescriber can actually pull. So we pulled the labels.
Do estradiol patch brands really differ? (Same dose, very different patch)
Yes — more than most people realize. At the same 0.05 mg/day dose, FDA-approved estradiol patches differ in wear schedule, patch size, and ingredients. Those differences give you real things to discuss with your prescriber. They do not prove which patch will be gentlest on your particular skin.
We read the current label for each patch below via DailyMed and lined them up at the same 0.05 mg/day dose. Product labels and marketing status verified July 14, 2026.
How selected U.S. estradiol patches compare at 0.05 mg/day
| Patch (0.05 mg/day) | Wear schedule | Patch area | Adhesive + notable ingredients |
|---|---|---|---|
| Minivelle (Noven, brand) | Twice a week | 3.30 cm² ← smallest | Acrylic + silicone adhesives; oleyl alcohol; dipropylene glycol; povidone |
| Dotti (Amneal, generic) | Twice a week | 3.78 cm² | Acrylic + silicone adhesives; oleyl alcohol; dipropylene glycol; povidone |
| Vivelle-Dot (Sandoz, brand) | Twice a week | 5.0 cm² | Acrylic + silicone adhesives; oleyl alcohol; dipropylene glycol; povidone |
| Climara (Bayer, brand) | Once a week | 12.5 cm² | Acrylate copolymer adhesive; fatty acid esters |
| Mylan estradiol, continuous-delivery (generic) | Once a week | 15.5 cm² ← largest | Pressure-sensitive acrylic adhesive; propylene glycol; povidone; colloidal silicon dioxide |
The finding worth remembering: at the same 0.05 mg/day dose, the patch ranges from 3.30 cm² (Minivelle) to 15.5 cm² (Mylan once-weekly) — the largest is about 4.7 times the size of the smallest. You can also see the ingredient split: propylene glycol — that recognized allergen — sits on the Mylan once-weekly label. The twice-weekly patches (Minivelle, Dotti, Vivelle-Dot) list oleyl alcohol instead.
What this table can’t do — and why we’re telling you
This comparison cannot tell you which patch caused your rash, and it cannot crown a “least irritating” patch — no label or study we found ranks them that way. What it cando is identify real formulation differences worth discussing. Instead of telling your clinician “the patch gives me a rash,” you can now say:
“I’m on the 15.5 cm² once-weekly generic with propylene glycol; would a smaller patch, or one without propylene glycol, make sense for me?”
That’s a question a clinician can act on.
Can I switch estradiol patch brands if one irritates my skin?
A different patch can have a different adhesive, different ingredients, a different size, or a different wear schedule, so switching is a reasonable thing to raise with your prescriber or pharmacist. It’s not a guaranteed fix, and you shouldn’t swap products or change your dosing schedule on your own. The first step is knowing exactly what you’re using now.
Find your exact product
On the box or pharmacy label, look for: the brand or generic name, the maker (manufacturer or 'labeler'), the strength, whether it says once-weekly or twice-weekly, and the NDC — the National Drug Code, a number that identifies the exact product. Snap a photo of all of it.
Ask your pharmacist what changed
A pharmacist can check the labeler and NDC on your current fill, and may be able to compare it with your previous fill. Try: "Can you tell me the manufacturer and NDC for this fill, and for my last fill? I got a patch-shaped reaction after this refill and I want to show my prescriber whether the product changed."
Ask your prescriber a specific question
Not 'help, rashes,' but: "Would a different FDA-approved estradiol patch — one with a different adhesive or ingredient list, or a smaller patch — be reasonable for me?"
Know that stock and insurance play a role
The product you get can depend on pharmacy stock, wholesaler supply, your insurer's or plan's rules, and your prescription. Your prescriber and pharmacist can work out what's both appropriate and available.
Why did the rash start after months — or right after a pharmacy change?
A reaction that appears after months of smooth sailing doesn’t rule out an allergy — sensitivities can develop after repeated exposure. And a pharmacy switch can quietly change your patch’s size, adhesive, or ingredients even when the prescription still reads “estradiol 0.05 mg/day.” Same words on the label, different patch on your skin.
You may have become newly sensitive
Contact allergies often build over time. You can use something for months, even years, and then your immune system decides it doesn’t like an ingredient. “I’ve used patches forever” doesn’t put an allergy off the table.
The product may have changed without the dose changing
Estradiol patches have had on-and-off supply shortages through 2024–2026, so pharmacies have been switching patients between manufacturers more than usual. If your pharmacy switched you, you could be wearing a bigger patch with different glue — even though nothing about your prescription changed.
Build a quick before-and-after record
| Track this | Old fill | New fill |
|---|---|---|
| Brand / manufacturer | Fill in from box/pharmacy label | Fill in from box/pharmacy label |
| NDC number | Fill in from box/pharmacy label | Fill in from box/pharmacy label |
| Dose & schedule | Fill in from box/pharmacy label | Fill in from box/pharmacy label |
| Where you applied it | Fill in from box/pharmacy label | Fill in from box/pharmacy label |
| How soon the rash started | Fill in from box/pharmacy label | Fill in from box/pharmacy label |
| Lot number & fill date | Fill in from box/pharmacy label | Fill in from box/pharmacy label |
| Photo taken? | Fill in from box/pharmacy label | Fill in from box/pharmacy label |
How should I apply the next patch to avoid another rash?
Once you’ve ruled out emergency and spreading reactions, product-specific application steps can cut down on avoidable friction and adhesion trouble — though they can’t prevent every irritant or allergic reaction. Follow your exact product’s instructions, because they vary.
- Rotate your spots. Don’t put a new patch where the last one was. Give a site time to recover before you use it again — many labels say at least a week.
- Start with clean, dry, intact skin. No lotion, oil, or powder on the exact spot. Never on skin that’s broken, burned, or already irritated.
- Avoid the waistline. Skip spots where a waistband or tight clothing will rub the patch all day; use an approved site instead.
- Press it on well. Press for the time your product’s label says — often about 10 seconds — especially around the edges, to get good contact and reduce lifting.
- Don’t apply to a rash. If a spot is still reacting, it’s off-limits. Use a different approved application site and ask your prescriber or pharmacist about timing.
Don’t cut or trim the patch.Cleveland Clinic’s estradiol-patch guidance says not to cut or trim these patches — cutting can change how the medicine is delivered, and it’s not how they’re meant to be used.
For leftover sticky residue,use your label’s method. Climara’s label says to let the area dry for about 15 minutes after removal, then gently rub it with an oil-based cream or lotion. That’s for after removal — it does not mean putting oil or lotion under a fresh patch.
Can I use hydrocortisone, Flonase, a barrier film, or Tegaderm under the patch?
These are popular internet tips, not standard estradiol-patch instructions — and that distinction matters. Anything you put under a patch can change how it sticks or how the drug absorbs. The safest answer is to ask your prescriber or pharmacist about your exact product before you try any of these.
Hydrocortisone cream
Treating an already-irritated spot after you remove a patch is different from putting steroid on the skin where your next patch goes, or under a patch. Ask what's appropriate for your specific reaction — don't freelance a routine.
Flonase (fluticasone) nasal spray on the skin
This is an off-label internet workaround, not a labeled instruction. Ask your clinician if it's even a reasonable idea for you before following any forum protocol.
Barrier films
A barrier might change contact or stickiness, and the effect can depend on the exact product. We won't promise it 'won't affect absorption,' because that depends on the specific patch.
Tegaderm or another overlay
Putting a film over a patch to help it stay put is not the same as putting a barrier between the medicine and your skin. The labels we reviewed don't give one universal rule on overlays — check with your pharmacist for your product.
Oral antihistamines
A pill is not a substitute for getting a spreading, blistering, or whole-body reaction actually evaluated.
Why won’t we just publish a hack?Because a tip can be all over the internet and still be wrong for your specific patch, your skin, your other medications, or your history. We’d rather hand you the right question to ask your pharmacist than a risky shortcut.
Should I remove an estradiol patch if it itches?
There’s no safe one-size answer — it depends on how bad it is, which product you’re using, and your other symptoms. Emergency signs mean act now. A mild, contained itch should be handled using your product’s instructions and your prescriber’s advice.
- Don’t let this question delay real care. Throat or breathing symptoms = 911 situation — not a “should I peel it off” question.
- Itch is not the same as a spreading or blistering reaction. A mild, contained itch is very different from a welt creeping outward or bubbling up.
- Never double up. If a patch bothered you or came loose, don’t overlap patches or shift your schedule on your own.
Ask your prescriber:
“My next patch is due on [date]. Given this reaction, should I apply it on schedule at a different approved spot, delay it, or switch to another product?”
Can a rash change estradiol absorption or make the patch stop working?
The look of a rash can’t tell you how much hormone you absorbed. Because labels tell you to apply patches to intact skin and give product-specific steps for a patch that lifts or falls off, damaged skin or poor sticking is a conversation for your prescriber or pharmacist — not something to fix by adding an extra patch.
- A rash doesn’t measure your hormone level. A redder or itchier reaction doesn’t mean you’re getting more or less estradiol.
- Lifting and a rash are separate issues. A patch can irritate while it’s still stuck on, or lift without causing an allergic reaction.
- Returning symptoms aren’t proof the patch “failed.” Whether to check hormone levels or adjust your dose is your clinician’s call — not something to reverse-engineer from a rash.
What if my skin can’t tolerate any estradiol patch?
A patch reaction usually doesn’t mean giving up estrogen — but it does depend on what’s clinically right for you. If systemic estrogen still fits your situation, a clinician can discuss another FDA-approved patch or a no-adhesive route, like a gel or spray, that delivers estradiol through the skin without the sticky patch.
FDA-approved estradiol options beyond the patch
| Option | What it is | Systemic or local | Sticky adhesive? | Route & safety note |
|---|---|---|---|---|
| Estradiol gel (EstroGel, Divigel, Elestrin; some generic) | A gel you rub on daily | Systemic | No | Transdermal. Let it dry and avoid transferring to others. May carry lower blood-clot risk than oral estrogen. |
| Estradiol spray (Evamist) | A metered spray | Systemic | No | Transdermal. Let dry at least 2 minutes before covering with clothing; keep site away from children until dry. |
| Estradiol pill (oral) | A daily tablet | Systemic | No skin contact | Oral estrogen passes through the liver, which raises clot risk more than transdermal routes. |
| Systemic vaginal ring (Femring) | A ring changed about every 90 days | Systemic | No skin adhesive | A systemic estradiol ring. Femring is systemic; Estring is local only and won't treat hot flashes. See our vaginal estrogen guide. |
One important safety point.A current or previous DVT, pulmonary embolism, stroke, or heart attack is listed as a contraindication in current systemic estradiol labeling — including patch labels (FDA label, DailyMed). A patch is not a “workaround” for a prior clot; if that’s your history, systemic estrogen may not be appropriate at all, by any route. Migraine and high triglycerides also need individual assessment.
| FDA-approved medication | Compounded medication |
|---|---|
| Made and labeled under FDA's approval and manufacturing rules | Prepared by a compounding pharmacy, outsourcing facility, or physician under compounding law — not FDA-approved |
| You can identify the exact approved product and read its label | Is not an FDA-approved generic and must not be described as equivalent to an FDA-approved drug |
| Reviewed by FDA for safety, effectiveness, and quality before marketing | FDA does not review compounded drugs for safety, effectiveness, or quality before marketing |
A patch rash alone doesn’t establish a need for a compounded product — talk through FDA-approved alternatives first when they can meet the clinical need. See our FDA-approved vs. compounded HRT guide.
If the patch route may not be for you, figure out your best next step first.
Find My HRT Path compares systemic vs. local care, FDA-approved vs. compounded options, insurance-based vs. cash-pay providers, and what’s available in your state.
Compare routes matched to my symptoms →What should I bring to my clinician or pharmacist?
Come with a photo, the product name, the manufacturer, the NDC, your dose, where you applied it, when the rash started, and whether it spread or stuck around after removal. The better your notes, the faster you get a real answer.
Bring to your pharmacist:
- Did the manufacturer change on my last refill?
- What are the inactive ingredients in this exact product?
- What does this label say to do if the patch lifts or falls off?
- Is an overlay allowed with this patch?
- Can you order the same manufacturer next time?
Ask your prescriber:
- Does this need an in-person look?
- Should I use my next scheduled patch, or wait?
- Would a different FDA-approved patch be reasonable?
- Would a no-adhesive route (gel or spray) fit my goals and history?
- Is dermatology or formal allergy patch testing worth it?
When a dermatologist helps:
If reactions keep coming back and no one can figure out why, ask about patch testing— a dermatology test that checks your skin against specific allergens. It can help identify a trigger, though a first round doesn’t always find it and more testing is sometimes needed (American Academy of Dermatology). It’s not needed for every little mark, but it’s the tool for a stubborn, repeating rash.
Estradiol patch rash: frequently asked questions
A rash’s appearance can’t reveal its exact cause or tell you what to do with your next dose — so these answers stay general, and point you to your clinician for the specifics.
The bottom line
A patch-shaped rash tells you where your skin was exposed — not which ingredient caused it. Rule out the emergency signs first. Then figure out whether it’s ordinary irritation or something that needs a closer look, document it, identify your exact product, and bring a sharp question to your clinician or pharmacist. If patches just aren’t friends with your skin, a gel, spray, or different formulation can often keep your treatment going — depending on what’s right for you. You have more options than “rash or nothing.”
Sources
Last verified: by The HRT Index Editorial Team. All label information from DailyMed (the FDA’s public label repository).
- MedlinePlus — Estradiol Transdermal Patch (skin-reaction and emergency signs; application guidance)
- American Academy of Dermatology — Contact dermatitis: signs and symptoms
- American Academy of Dermatology — Patch testing
- Minivelle — FDA label via DailyMed (area and ingredients at 0.05 mg/day)
- Dotti — FDA label via DailyMed (area and ingredients at 0.05 mg/day)
- Vivelle-Dot — FDA label via DailyMed
- Climara — FDA label via DailyMed
- Mylan estradiol transdermal, continuous-delivery once-weekly — FDA label via DailyMed
- JAAD Case Reports (2021) — allergic contact dermatitis to propylene glycol in a transdermal estradiol patch
- Cleveland Clinic — Estradiol Skin Patches (do not cut; application)
- FDA — Compounding and the FDA: Questions and Answers
Update history
— Published. Verified all patch labels via DailyMed; confirmed ingredient and size comparisons at 0.05 mg/day; checked marketing status with manufacturers.
Educational information from The HRT Index. Not medical advice, and not medically reviewed by a clinician. Always follow your prescriber’s and pharmacist’s guidance for your specific medication. See our corrections policy.
Still not sure which HRT program is right for you?
Take our free 90-second Find My HRT Path quiz to see your best-fit online care route, why it fits, and two backup routes — matched to your symptoms, history, and state, before your next consult.
Find My HRT Path → (free, ~90 seconds)Find My HRT Path doesn’t diagnose a rash and isn’t for emergencies.