How Long Does Vaginal Estrogen Take to Work?
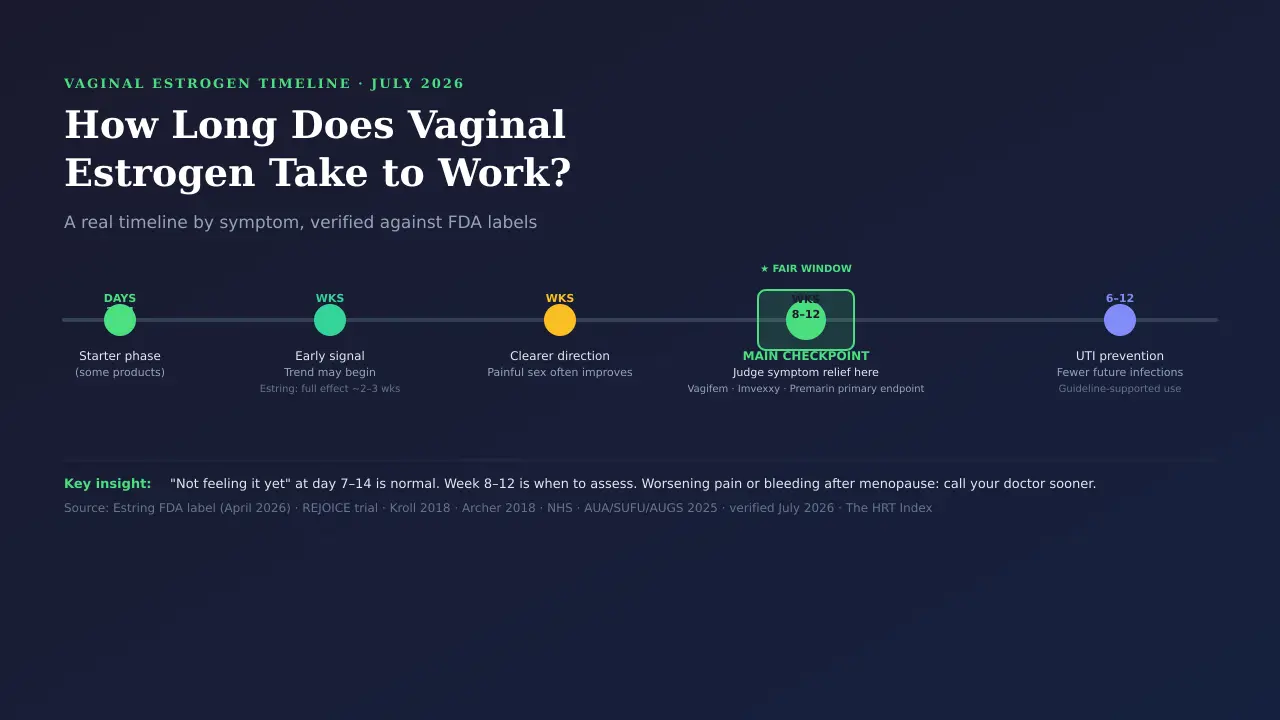
Short answer:Improvement often starts within a few weeks. Estring’s current FDA label says its full effect may take about 2 to 3 weeks; several other products used 12 weeks as the main study checkpoint, and the NHS says full benefit can take up to 3 months. Fewer recurrent UTIs is a separate, slower payoff — judged over months, not days.
Read this before anything else
Most of the time, early on, “nothing yet” is still within the normal window — but do not sit and wait if you have bleeding after menopause, rapidly worsening or severe pain, or signs of a urinary infection. Any bleeding after menopause needs prompt evaluation. Fever or chills, blood in your urine, or pain in your back or side below the ribs along with urinary symptoms calls for urgent medical attention.
| Where you are | What it usually means |
|---|---|
| First 2 weeks | Still early. In one insert study, some women improved by week 2 — but no relief this soon is not failure. |
| Weeks 2–4 | A trend may begin. Estring's label puts full effect around 2–3 weeks; one cream trial saw less itching and irritation by week 4. |
| Weeks 4–8 | The direction gets clearer. In that same cream trial, painful sex improved by week 8. |
| Weeks 8–12 | The strongest checkpoint across the major product studies. Judge symptom results here, not on day 10. |
| Over 6–12 months | The window used in studies for preventing repeat UTIs — measured in fewer future infections. |
This page is for you if:
You’re using (or about to start) prescribed low-dose local vaginal estrogen for menopause-related dryness, irritation, painful sex, or urinary symptoms, and you want a realistic timeline and a plan.
This is not a “wait and see” guide if:
You might have an active UTI, you have new bleeding after menopause, your pain is severe or worsening, or you’re hoping vaginal estrogen will fix hot flashes, night sweats, mood, or sleep — low-dose local estrogen won’t.
We’re The HRT Index — the independent decision resource for online menopause and HRT care. This article has no provider affiliate links. New to this treatment altogether? Start with our plain-language guide to what vaginal estrogen is, what it treats, and its safety context. Our free Find My HRT Path tool may later recommend providers we have affiliate relationships with — always disclosed.
How long does vaginal estrogen take to work for most symptoms?
Improvement can begin within a few weeks, but the fair window to judge low-dose vaginal estrogen depends heavily on the exact product and symptom. Estring’s current FDA label estimates full effect at about 2 to 3 weeks; several other product studies used week 12 as their main checkpoint, and the NHS says full benefit can take up to 3 months. Preventing recurrent UTIs is a slower, months-long goal.
Let’s clear up what “work” even means, because that one word is hiding four different finish lines. Low-dose local vaginal estrogen doesn’t work like a numbing medicine. It acts on estrogen-sensitive tissue in the vagina and lower urinary tract, gradually changing the tissue lining, the vaginal pH (acidity), and how your symptoms feel. So “working” can mean any of these:
- Your vaginal pH and cell health shift back toward pre-menopause levels (a lab measure).
- A symptom score drops — less dryness, less burning.
- Pain with sex decreases.
- You get fewer UTIs over time.
Those are four different clocks. That’s the whole reason the internet can’t agree on a single number.
The five timing windows
Think of it as phases, not one deadline:
- Days 1–14.Some tablets and inserts use a daily “starter” phase here. Products differ, though — creams follow their own schedules, and the Estring ring has no daily phase at all. Use the exact instructions for your product.
- Weeks 2–4.For many women this is when a trend starts. Estring’s label puts full effect around 2–3 weeks.
- Weeks 4–8. The direction becomes easier to feel. Painful sex often improves in this stretch.
- Weeks 8–12.The main checkpoint. If you’ve used it consistently and still feel nothing, this is when a check-in makes sense.
- Months 6–12. The window studies use to judge fewer repeat UTIs.
Why 8 to 12 weeks is a defensible answer
The big product studies keep landing on week 12as the point where they measure whether the medicine worked. The estradiol tablet (Vagifem), the estradiol softgel insert (Imvexxy), and Premarin Vaginal Cream all used a 12-week main checkpoint in the studies behind their FDA labels. That makes week 12 a solid cross-product research checkpoint — but it’s a study design choice, not a universal biological deadline, and it doesn’t guarantee any individual result.
Could you feel better sooner? Absolutely. Many women do, and Estring’s own label says full effect may come around 2–3 weeks. But “the study measured it at week 12” and “some women feel it earlier” are both true. One is the stronger checkpoint; the other is an early, product-specific signal.
What does the evidence show by symptom, product, and week?
The HRT Index Vaginal Estrogen Evidence Clock — v1.0 · evidence checked
The table below separates three things most pages blur together: the earliest signal a real study found, the stronger checkpoint where results are judged, and what that means for you. We built it because nearly every page we found gives you a confident calendar without showing where the numbers come from. Ours shows the receipts.
| What you’re tracking | Earliest signal in research | Stronger checkpoint | What it means for you |
|---|---|---|---|
| Vaginal pH and cell changes | Week 2 in the REJOICE estradiol-insert trial (a secondary result) | Week 12 (the repeated primary endpoint for Vagifem, Imvexxy, and Premarin cream) | Your tissue can be healing before you feel fully better. Week 2 is a head start from one product, not a deadline. |
| Dryness | Improved by week 4 in one 0.003% estradiol-cream (Archer) dryness trial | Week 12 endpoint; NHS says full benefit up to 3 months | Dryness often eases early, but "full" can take longer. Some feel it within weeks; some take months. |
| Itching / irritation | Improved by week 4 in a separate 0.003% estradiol-cream (Kroll) dyspareunia trial | Week 12 | Surface irritation frequently improves early. Worsening irritation is a reason to get checked, not to add doses. |
| Painful sex (dyspareunia) | As early as week 2 for the estradiol insert; by week 8 in the Kroll cream trial | Week 12 across multiple product studies | It can start early, but give it the fuller window — tissue needs both thickness and stretch to return. |
| Urinary symptoms with Estring | Estring's current FDA label: about 2–3 weeks for full vaginal and urinary effect | Older comparison studies also reported outcomes at 12 weeks | The 12-week study visit isn't the same as the label's product-specific estimate. Possible UTI symptoms still need separate evaluation. |
| Fewer recurrent UTIs | Not an immediate-relief goal | Measured over roughly 24 weeks to a year | Prevention is judged in fewer future infections. It does not treat an infection you have now. |
| When markers move but you don't | In one pragmatic trial (Mitchell 2018), a 10-mcg estradiol tablet was not better than placebo on the most bothersome symptom at 12 weeks, even though pH and cell measures improved more | — | Lab changes and how you feel don't always move together. Response varies from person to person. |
| Hot flashes, night sweats, sleep, mood | No local-treatment timeline | Not applicable | Low-dose local vaginal estrogen is not built for whole-body symptoms. You'll need a different path. |
These studies used different formulations, doses, symptoms, and endpoints, so this is an evidence map — not a pooled success rate, a head-to-head speed ranking, or a promise that everyone responds on the same schedule.
The honest bottom line: Week 2 is an early signalfrom specific research. Estring’s label says around 2–3 weeks. Week 12 is the strongest cross-product checkpoint. And UTI prevention is a months-long story. Anyone giving you an exact day for every symptom is guessing.
Not sure if your current route or provider fits your situation?
Find My HRT Path matches your symptoms to the right care — and flags when online care isn’t the right starting point.
See how Find My HRT Path works →Free · no email required · The HRT Index may earn a commission if you choose an affiliated provider.
How does the vaginal-estrogen timeline differ by symptom?
There’s no dependable one-size-fits-all order. Different product trials found different early signals: painful sex improved by week 2 with one softgel insert, dryness improved from week 4 in one 0.003% estradiol-cream trial, and itching and irritation improved by week 4 in a separate 0.003% cream trial. Recurrent-UTI prevention stays the slowest, because it’s measured in fewer future infections over months.
Vaginal dryness
Dryness often eases early. In a 0.003% estradiol-cream trial focused on dryness (Archer 2018), dryness improved from week 4 through week 12, and the NHS notes full benefit can take up to 3 months — so a few weeks to a few months is normal. One honest note: even when dryness improves, a lubricant or vaginal moisturizer can still help alongside vaginal estrogen when you need it.
Itching, burning, and irritation
These frequently improve early too. In a separate 0.003% estradiol-cream trial (Kroll 2018, focused on painful sex), women reported significantly less vaginal and vulvar itching and irritation by week 4versus placebo. But burning has more than one cause. If it’s getting worse, comes with unusual discharge or odor, or shows up with urinary symptoms, that’s a reason to get checked — not a reason to double up on cream.
Painful sex (dyspareunia)
Dyspareunia is the medical word for painful sex, and it has the most study data. In the REJOICE trial of an estradiol softgel insert (Imvexxy), some women had less pain as early as week 2— though the main measurement point was week 12. In the Kroll cream trial, painful sex improved by week 8. So the range is real: it can start early, but the fuller result usually lands closer to 8 to 12 weeks. If sex still hurts after a consistent 12 weeks, that’s worth a conversation, because pain can also come from pelvic-floor tension, a skin condition, or infection — not just low estrogen.
Urinary urgency, frequency, and painful peeing
This one needs care. Estring’s current FDA label says its full effect on vaginal and urinary symptoms may take about 2 to 3 weeks; older comparison studies also reported outcomes at 12 weeks. But urgency, frequency, and burning when you pee overlap heavily with a UTI.
Fewer recurrent UTIs
This is where vaginal estrogen quietly shines — but slowly. The 2025 joint AUA/SUFU/AUGS guideline on genitourinary syndrome of menopause recommends low-dose vaginal estrogen to lower the risk of futurerecurrent UTIs in appropriate women after menopause. Two important caveats: lowering that risk is a guideline-supported use, not an FDA-approved urinary indication for these low-dose local products — and none of them treat an infection you already have. Judge prevention over months, not days. For a full overview, see our page on vaginal estrogen for recurrent UTIs.
Does the cream, tablet, insert, or ring work faster?
There isn’t good evidence that any one form is universally faster. Different products were studied on different symptoms with different endpoints, so they can’t be lined up for a fair race — and Estring’s own label reports it worked about as well as a conjugated-estrogen cream at 12 weeks, not clearly faster. Pick the form you’ll actually use consistently, because using it as prescribed is one of the biggest factors in whether it helps. See our vaginal vs. systemic estrogen guide for the bigger picture.
| Form (examples) | Typical label routine* | What the evidence shows | What you can’t conclude |
|---|---|---|---|
| Estradiol cream 0.01% (Estrace, generic) | Often 2–4 g daily for 1–2 weeks, then gradually reduced; maintenance often ~1 g one to three times weekly | Studied FDA-approved cream regimen | That a 0.003% research cream's exact timing applies to this 0.01% product. |
| Premarin Vaginal Cream | Depends on the indication — e.g., a 21-days-on/7-off schedule, or 0.5 g twice weekly for painful sex | Studied on its own regimen; week-12 primary endpoint | That its schedule or results transfer to every other cream. |
| Vaginal tablet / softgel insert (Vagifem, Yuvafem, Imvexxy) | One insert daily for 2 weeks, then twice weekly | Week 12 primary endpoint; insert saw some pain relief by week 2 | That tablets are "slower" — earlier weeks just weren't the headline. |
| Estring ring (7.5 mcg/day) | One ring placed in the upper third of the vagina, left in for 90 days | Label: about 2–3 weeks to feel full effect; comparison studies also assessed 12 weeks | That the ring beats creams on speed — comparisons found similar 12-week results. |
*These are label examples, not instructions for you. Follow the exact prescription and current label for your product.
Does every product have a two-week daily “starter” phase?
No — the schedules differ meaningfully by product:
- Tablets and softgel inserts (Vagifem, Yuvafem, Imvexxy):Yes — one insert daily for 2 weeks, then twice weekly. This is the loading phase in their current labels.
- Estradiol cream 0.01% (Estrace):Yes, but tapered differently — often daily for 1–2 weeks, then gradually reduced to maintenance. Your exact prescription may vary.
- Premarin Vaginal Cream:It depends on the indication. The label uses different schedules for different symptoms — there’s no single “two-week” rule across indications.
- Estring: No daily starter phase at all. You insert one ring and leave it in place for 90 days. The timeline is continuous, not phased.
If your prescriber’s instructions differ from what’s on the label, follow your prescriber. And if you’re unsure which phase you’re in, your pharmacist can walk you through it.
What does “working” actually look like day to day?
Look for a direction, not a miracle. Working usually looks like: less daily dryness or burning, fewer painful episodes, more comfort with touch or sex, or less urinary urgency over time. Because the change is gradual, it can be hard to remember accurately week to week — which is exactly why a simple log helps.
Rate one or two things, once a week
Pick your most bothersome symptom and score it 0 (none) to 10 (worst) once a week — same day, same time. Day to day, you’ll see noise. Week to week, you’ll see the trend.
Weekly log to bring to your clinician:
Week #:
Product & how often used:
Main symptom:
Score last week (0–10):
Score this week (0–10):
Better / same / worse?
Any bleeding, UTI signs, or new pain?
Questions for my clinician:
This 0–10 log is an editorial tracking aid to document your trend for a clinician conversation — not a validated medical scale, and not a substitute for your prescribed follow-up.
One thing notto do: don’t try to measure your own vaginal pH at home as “proof.” pH and cell measures are used in research and sometimes in clinical assessment, but a home pH strip can’t prove treatment is working or explain why symptoms persist. Your symptoms and your weekly trend are what matter to you.
What if it’s not working after 2 weeks, 6 weeks, or 3 months?
At 2 weeks, no relief is usually too early to call it a failure. By 6 weeks, the trend tells you more. At about 3 months, the NHS advises talking to your doctor if you’re not better — the diagnosis, the product, how you’re using it, or another cause may need a fresh look. The move is almost never to quietly change your own dose.
| Where you are | What it may mean | What to do |
|---|---|---|
| Nothing after a few days | Too early to judge. | Keep using it exactly as prescribed. |
| Nothing at 2 weeks | Still normal — early signals come from specific products, not a universal deadline. | Double-check you understand the instructions. Don't add doses on your own. |
| Some change at 4–6 weeks | A trend is forming. | Keep tracking the same symptom week to week. |
| No trend at 6–8 weeks | Not necessarily failure, but reasonable to message your prescriber — sooner if it's worsening. | Prepare questions (below). |
| No improvement at ~12 weeks / 3 months | The right time to reassess. | Contact your clinician rather than waiting indefinitely. |
| Another suspected UTI while using it | Prevention isn't perfect and doesn't treat an active infection. | Get the UTI evaluated now. Don't wait for estrogen. |
| Symptoms are worse | Could be irritation, infection, or another cause. | Contact your clinician sooner. |
Questions to bring to your clinician
- Is my main symptom one vaginal estrogen is expected to treat?
- Could an infection or another vaginal, urinary, or pelvic-floor issue be involved?
- Is this the right form for where my symptoms are?
- Am I using it correctly?
- What improvement should we expect by my next visit?
- When should we consider a different treatment or a referral?
If your route or provider never fit your situation, that’s fixable.
Our free Find My HRT Path tool turns your symptoms and situation into a personalized action plan — and flags when online care isn’t the right starting point.
Could my symptoms be caused by something other than low estrogen?
Yes — and this matters. Dryness, burning, pain, discharge, and urinary symptoms overlap with infections and other vaginal, vulvar, urinary, and pelvic-floor conditions. So “it’s not working” doesn’t automatically mean the medicine failed. It can mean the target was wrong.
Things a clinician might consider (examples, not a self-diagnosis checklist): a UTI, a yeast or bacterial infection, contact irritation from a product, a vulvar skin condition, pelvic-floor dysfunction, vulvodynia, overactive bladder, or another cause of bleeding.
GSM and a UTI can bothcause burning, urgency, and frequency. But fever, chills, cloudy or bloody urine, or back/side pain point toward infection and shouldn’t be passively watched. A web page can’t diagnose why your symptoms persist. What it cando is help you recognize when “how long does it take” is no longer the right question, and “what else could this be” is.
What symptoms will low-dose local vaginal estrogen NOT treat?
Low-dose local vaginal estrogen is designed for vaginal and nearby urinary symptoms — dryness, irritation, painful sex, and some bladder symptoms, plus lowering the risk of recurrent UTIs. It is not a general treatment for hot flashes, night sweats, mood changes, or sleep problems, because very little of it reaches the rest of your body. Matching your main symptom to the right treatment saves you weeks of waiting on the wrong one.
| Usually a job for local vaginal estrogen | Usually needs a different path |
|---|---|
| Vaginal dryness | Hot flashes |
| Vulvar/vaginal irritation from GSM | Night sweats |
| Painful sex from tissue changes | Mood changes |
| Some GSM-related urinary symptoms | Sleep disruption |
| Lowering recurrent-UTI risk | Whole-body symptom control |
The honest catch:Vaginal estrogen is not a fast fix, and low-dose local products are not built to treat whole-body menopause symptoms. That sounds like a downside. It’s actually the design. Because the dose is low and mostly stays local, systemic exposure is much lower than with pills or patches — which is why major guidance evaluates recommended low-dose local products differently from systemic hormone therapy. For the right symptom, that gentle, local design is exactly what you want.
If the thing you’d most like to fix is on the “different path” side of that table — hot flashes, night sweats, sleep, mood — waiting longer on a local cream won’t get you there.
Find My HRT Path matches your symptom pattern to local, systemic, non-hormonal, or in-person care.
Match my symptoms to the right path →Free · ~90 seconds · no email · The HRT Index may earn a commission if you choose an affiliated provider.
Is low-dose local vaginal estrogen absorbed into the body?
Some estrogen is absorbed — it’s not zero — but with recommended low-dose local products the amount reaching your bloodstream is much lower than with estrogen used to treat hot flashes. Estring’s own FDA label states that systemic absorption occurs, while noting the exposure is generally lower than systemic estrogen products. That lower exposure is why major guidance evaluates these products differently from systemic therapy; it does not make any product risk-free, and product-specific warnings and bleeding guidance still apply.
For more on this topic, see our guide to whether vaginal estrogen is safe long term and our side effects overview.
Do you need progesterone with it?
For recommended low-dose localvaginal estrogen, routine progesterone generally isn’t needed the way it is with systemic estrogen in a woman with a uterus. That’s different for a systemicvaginal product like Femring. The exact product, dose, any systemic hormones you also take, your bleeding history, and your clinical plan all matter, and long-term (beyond one year) endometrial-safety data for low-dose vaginal estrogen are limited — so your prescriber tailors this to you.
What about a history of breast cancer?
For someone with a history of estrogen-dependent breast cancer, ACOG recommends starting with non-hormonal options. If those don’t relieve symptoms enough, low-dose vaginal estrogen may be considered through shared decision-making — and if you take an aromatase inhibitor, that conversation should include your oncologist. See our detailed overview on vaginal estrogen after breast cancer. This is a decision to make with your care team, not from an article.
What changed in FDA vaginal-estrogen labeling in 2025–2026?
In November 2025, the FDA moved to remove specific boxed-warning language from menopausal hormone therapy labeling after reviewing the scientific literature. On , it approved the first six updated labels — and one of them was Estring, a vaginal estrogen product. This changed class-warning language; it was not a declaration that every vaginal estrogen product is risk-free or that every label had already been updated.
- November 10, 2025— the FDA announced it would remove boxed-warning language about cardiovascular disease, breast cancer, and probable dementia from menopausal hormone therapy products, including local vaginal products.
- February 12, 2026— the FDA approved the first batch of six updated labels: Prometrium, Divigel, Cenestin, Enjuvia, Estring (the vaginal one), and Bijuva.
- The endometrial (uterine) cancer warning stays on systemic estrogen-alone products.
- As of , Estring was the only topical vaginal estrogen product on the FDA’s published updated-label list. The FDA may add more products as further label changes are approved.
Should you keep using it once it starts working?
Generally, yes — the benefit lasts only as long as you use it. Vaginal estrogen manages an ongoing condition; it doesn’t cure it. The NHS notes symptoms can return if you stop, so many women continue low-dose local vaginal estrogen for an extended period. How long, and how often to reassess, is an individual decision — The Menopause Society says low-dose vaginal estrogen may be considered at any age and for extended duration when needed, and the NHS recommends ongoing review.
A reassuring note if you’re starting late: the cited guidance doesn’t set an age cutoff for low-dose local vaginal estrogen, so it’s not automatically “too late.” A person starting later still needs an individualized look at symptoms, any contraindications, bleeding, and goals. And if you ever want to stop, talk to your prescriber first — the NHS says a clinician may suggest reducing treatment gradually, since symptoms can return.
How did The HRT Index verify this timeline?
We built this under The HRT Index Verification Standard — reading primary sources, separating FDA-approved from compounded, and re-checking on a fixed schedule. For this page, that meant checking FDA-approved product labels on DailyMed, the actual trial timepoints behind them, and current guidance from the FDA, the NHS, The Menopause Society, ACOG, and the AUA. Then we did the part most pages skip: we separated early study signals from label estimates, from primary endpoints, from our own editorial reading.
What we actually verified ()
- Estring’s current FDA label estimate of about 2–3 weeks to full vaginal and urinary effect, its upper-third placement, and its 7.5 mcg/day dose.
- Week-12 primary endpoints in current FDA labeling for Vagifem, Imvexxy, and Premarin Vaginal Cream.
- The REJOICE insert trial: reduced painful sex as early as week 2 (a secondary result), with week 12 as the primary endpoint.
- Two separate 0.003% estradiol-cream trials — the Kroll dyspareunia-focused trial (itching/irritation improved at week 4, painful sex at week 8, dryness at the week-12 endpoint) and the Archer dryness-focused trial (dryness improved from week 4 through week 12).
- The Mitchell 2018 pragmatic trial, where a 10-mcg estradiol tablet was not superior to placebo on the most bothersome symptom at 12 weeks despite stronger pH and cell changes.
- NHS guidance that full symptom benefit can take up to 3 months.
- AUA/SUFU/AUGS 2025 guidance recommending low-dose vaginal estrogen to reduce future recurrent-UTI risk (a guideline-supported use, not an FDA urinary indication).
- The FDA’s boxed-warning removal timeline (initiated Nov 10, 2025; first six labels approved Feb 12, 2026, including Estring).
What we did NOT claim
- That one form is fastest for every woman.
- That relief reliably begins on an exact day.
- That compounded products are equivalent to FDA-approved ones.
- That you should change your prescribed dose, schedule, or placement based on this article.
- A specific diagnosis for anyone’s ongoing symptoms.
See something that’s changed, or a source we should review? Use the corrections address in our footer. Material changes get logged and dated.
Frequently asked questions
Most timing questions come down to one idea: an early change can show up in weeks, but the fairest reassessment point is usually closer to 8 to 12 weeks — and the exact number depends on the product. The right next step changes when symptoms are worsening, look like an infection, fall outside what local vaginal estrogen treats, or haven’t budged by about three months.
Can vaginal estrogen work in a few days?
A few days is too early to judge. Some women perceive small changes quickly, but that doesn’t reflect the expected timeline — and it’s not a reason to change how you’re using it.
How long does vaginal estrogen cream take to work?
In a 0.003% estradiol-cream trial, itching and irritation improved by week 4, painful sex by week 8, and dryness was measured at the week-12 endpoint. Don’t assume the same exact timing for every cream — FDA-approved products like Estrace (0.01%) and Premarin cream have their own regimens — but a few weeks to about three months is realistic.
How long does vaginal estrogen take to work for dryness?
Often a few weeks for early relief, with fuller benefit by around 8 to 12 weeks; the NHS says up to 3 months. A lubricant or moisturizer can help alongside it when needed.
How long does vaginal estrogen take to work for painful sex?
It ranges. An estradiol insert study saw some relief as early as week 2, a cream study saw it by week 8, and multiple product studies judged results at week 12. Give it the fuller window before deciding it isn’t helping.
How long does vaginal estrogen take to help urinary frequency?
It depends on the product. Estring’s current FDA label estimates full vaginal and urinary effect at about 2–3 weeks, while older comparison studies reported outcomes at 12 weeks. Urinary frequency also has causes beyond menopause — get it checked if it’s persistent or worsening.
How long does vaginal estrogen take to prevent UTIs?
Judge prevention over months, not days. Studies count fewer future infections over periods like 24 weeks or a year. It does not treat an active UTI, and it’s a guideline-supported use rather than an FDA-approved urinary indication.
I finished the two-week daily phase and feel no different. Did it fail?
Not necessarily — two weeks is early, and not every product even uses a daily phase. Keep following your prescription rather than restarting or extending it on your own, and contact your prescriber if symptoms are worsening or there’s still no trend as you near the 8-to-12-week mark.
Does missing a dose reset the timeline?
There’s no single answer, because instructions differ by product. Follow the missed-dose guidance in your product information or ask your pharmacist — and don’t double up to “catch up.”
What if it makes me feel worse?
Contact your prescriber sooner rather than waiting three months. Worsening symptoms can mean irritation, an infection, another condition, or a treatment issue.
Does low-dose vaginal estrogen help hot flashes or night sweats?
No. Low-dose local vaginal estrogen reaches the bloodstream in only tiny amounts, so it isn’t a treatment for hot flashes or night sweats, which usually need systemic care. (Femring, a systemic vaginal ring, is a separate story.)
Does Femring follow the same timeline as low-dose local vaginal estrogen?
No. Femring is a systemic vaginal ring approved for hot flashes as well as vaginal atrophy. Its dosing, its systemic estrogen exposure, its progesterone considerations, and its safety picture are not the same as Estring, vaginal tablets, softgel inserts, or low-dose local creams.
Do I need progesterone with vaginal estrogen?
For recommended low-dose local vaginal estrogen, routine progesterone generally isn’t required the way it is with systemic estrogen in a woman with a uterus. This does not apply to systemic products like Femring, and long-term endometrial-safety data are limited — so confirm your plan with your clinician.
How long after using vaginal estrogen can I have sex?
It’s product-specific — follow your product’s instructions. Estring can generally stay in place during sex and may be removed briefly if it’s uncomfortable; creams, tablets, and inserts have their own timing and application instructions.
Can I use low-dose vaginal estrogen together with systemic HRT?
Sometimes. Systemic estrogen improves vaginal symptoms for many women, but some with lingering symptoms also use a low-dose vaginal product under their clinician’s plan. That’s an individualized combination, not a schedule to build from an article.
Can vaginal-estrogen cream affect condoms or diaphragms?
Some vaginal creams and gels can damage latex condoms or diaphragms. Check the current instructions for your exact product, and ask a pharmacist when barrier contraception or STI protection matters.
Can I use vaginal estrogen long term?
Usually, yes. Symptoms tend to return if you stop, and duration is an individual decision to make with your prescriber — guidance supports extended use when needed, with ongoing review.
I’ve had breast cancer or take an aromatase inhibitor — can I use it?
ACOG recommends non-hormonal options first for people with a history of estrogen-dependent breast cancer; if those don’t help enough, low-dose vaginal estrogen may be considered through shared decision-making, and an aromatase inhibitor means involving your oncologist. Please make this decision with your care team.
The bottom line
Vaginal estrogen can start producing real changes within a few weeks — Estring’s label even puts its full effect around 2 to 3 weeks — but 8 to 12 weeks is the fair window to judge symptom relief across products, and the NHS says full benefit can take up to 3 months. Preventing repeat UTIs takes longer, on the order of months. And worsening pain, bleeding after menopause, or signs of infection deserve attention sooner, not later.
Still early
No change at day 7 or 14 is not failure.
Time to check in
Little or no improvement around 12 weeks or 3 months.
Don’t wait
Worsening pain, bleeding after menopause, or infection signs.
Still not sure whether local, systemic, non-hormonal, or in-person care fits your situation?
Find My HRT Path
Free, roughly 90-second matching quiz. Personalized action plan — and a heads-up when online care isn’t the right first step — before your next consult.
Start the free quiz →No email required. The HRT Index may earn a commission if you choose an affiliated provider.
Sources
- 1.NHS — Common questions about vaginal oestrogen and How and when to use vaginal oestrogen (full benefit can take up to 3 months; symptoms may return after stopping; creams/gels can affect condoms and diaphragms). Accessed July 2026; page last reviewed 27 January 2023. www.nhs.uk
- 2.Estring (estradiol vaginal system) — FDA label via DailyMed (2 mg estradiol releasing 7.5 mcg/day over 90 days; upper-third placement; full vaginal and urinary effect in about 2–3 weeks; label revised April 2026). dailymed.nlm.nih.gov
- 3.Imvexxy (estradiol vaginal insert) — FDA label via DailyMed (one insert daily for 2 weeks then twice weekly; week-12 primary endpoints). REJOICE trial: Constantine GD, et al. Menopause. 2017;24(4):409–416. Early-onset analysis: PubMed 31688572. dailymed.nlm.nih.gov
- 4.Vagifem (estradiol vaginal tablet) — FDA label via DailyMed (week-12 primary endpoint). dailymed.nlm.nih.gov
- 5.Premarin Vaginal Cream — FDA label via DailyMed (indication-specific regimens; week-12 assessment). dailymed.nlm.nih.gov
- 6.Kroll R, Archer DF, Lin Y, et al. Estradiol vaginal cream 0.003% in postmenopausal women with dyspareunia as the most bothersome symptom. Menopause. 2018;25(2):133–138. PMID 28926514 (itching/irritation improved at week 4, painful sex at week 8, dryness at the week-12 endpoint). pubmed.ncbi.nlm.nih.gov
- 7.Archer DF, Kimble TD, Lin FDY, et al. Estradiol vaginal cream 0.003% in postmenopausal women with vaginal dryness as the most bothersome symptom. J Womens Health. 2018;27:231–237. PMID 29193980 (dryness improved from week 4 through week 12). pubmed.ncbi.nlm.nih.gov
- 8.Mitchell CM, Reed SD, Diem S, et al. Vaginal estradiol or vaginal moisturizer vs placebo for postmenopausal vulvovaginal symptoms: a randomized clinical trial. JAMA Intern Med. 2018;178:681–690 (10-mcg estradiol tablet not superior to placebo on the most bothersome symptom at 12 weeks). pubmed.ncbi.nlm.nih.gov
- 9.AUA/SUFU/AUGS — Genitourinary Syndrome of Menopause Guideline (2025) (low-dose vaginal estrogen recommended to reduce recurrent-UTI risk; reassess after starting; long-term follow-up). auanet.org. www.auanet.org
- 10.The Menopause Society — 2022 Hormone Therapy Position Statement and GSM MenoNote (low-dose vaginal estrogen; routine progestogen generally not indicated with recommended low-dose local therapy; may be considered at any age/extended duration). menopause.org. menopause.org
- 11.ACOG — Treatment of Urogenital Symptoms in Individuals With a History of Estrogen-Dependent Breast Cancer (2021) (non-hormonal first-line; low-dose vaginal estrogen via shared decision-making; aromatase-inhibitor decisions involve the oncologist). acog.org. www.acog.org
- 12.FDA & HHS — menopausal hormone therapy labeling changes (boxed-warning removal initiated Nov 10, 2025; first six labels approved Feb 12, 2026, including Estring; endometrial warning retained for systemic estrogen-alone). fda.gov; hhs.gov. www.fda.gov
- 13.FDA — Compounding: Questions and Answers (FDA does not review compounded drugs before marketing for safety, effectiveness, or quality). fda.gov. www.fda.gov
- 14.Femring (estradiol acetate vaginal ring) — FDA label (systemic ring approved for moderate-to-severe vasomotor symptoms and vulvar/vaginal atrophy). accessdata.fda.gov. www.accessdata.fda.gov
Reader-question language on this page reflects common themes in public menopause discussions and is included to reflect what women are asking — never as medical, safety, or regulatory evidence.
Last updated: · Last verified:
The HRT Index reviews this page on a fixed schedule (top items monthly, full roster quarterly). Update dateModified only on substantive change. Submit via IndexNow on every update.