HRT for Perimenopause Heavy Periods: What Actually Works
HRT for perimenopause heavy periods can help — but usually not the way people expect, and rarely estrogen on its own. ACOG says hormone therapy can ease heavy bleeding during perimenopause, and periods often get lighter and more predictable on it. But estrogen by itself can make bleeding worse, no menopausal HRT is FDA-approved specifically for heavy bleeding, and unexplained heavy bleeding has to be checked before you start. Here is what actually works — and the one lab nobody orders.
This page is for you if you are roughly 40 to 55, still getting periods, they have turned heavy or unpredictable, and you are trying to work out whether HRT is the answer.
This page is not for you ifyou have gone 12 months or more without a period and you are bleeding now. That is postmenopausal bleeding — a different situation with a different urgency, and it needs a doctor this week whether or not you are on HRT. Read about bleeding after menopause and after starting HRT
Or if your periods have gone irregular in timing but the flow is normal. Different problem, different risk profile. Read the irregular periods page
The HRT Index is the independent decision resource for online menopause and HRT care — comparing telehealth providers on clinical legitimacy, care quality, medication fit, price transparency, and access, with every claim verified and dated.
Does HRT for perimenopause heavy periods actually work?
Sometimes — but the details decide everything. ACOG says hormone therapy can help heavy menstrual bleeding during perimenopause, and periods often become lighter and more predictable on it. The catch: estrogen on its own can make heavy bleeding worse, no menopausal HRT product is FDA-approved specifically for heavy bleeding, and new unexplained bleeding needs to be evaluated before systemic estrogen is started or changed.
When people say HRT helped their heavy periods, what usually helped is the progesterone sideof the treatment — a progestogen, or a hormonal IUD — not the estrogen. That distinction is the whole story on this page.
Here is what is true, stated plainly:
- Hormone therapy can be part of the answer. ACOG says so directly. If you have heavy bleeding and hot flashes, a well-chosen regimen can treat both.
- Estrogen alone can backfire.Adding estrogen without enough progestogen can thicken the lining further and make bleeding heavier — the opposite of what you want.
- No menopausal HRT product is FDA-approved specifically to treat heavy periods. Some hormonal products areapproved for heavy bleeding — just not the menopausal-symptom ones. We name every one below.
- Unexplained heavy bleeding has to be worked up first. This is printed on the drug labels.
“But my friend’s HRT made her periods lighter”
She is probably right. Some HRT regimens are builtto produce a bleed on a schedule — sequential HRT, with estrogen through the month and a progestogen added for part of it. Going from unpredictable flooding to a predictable monthly bleed can genuinely feel like a fix. But making bleeding predictable and treating heavy bleedingare two different jobs. Her regimen worked because of how the progestogen was managed — not because estrogen fixes heavy periods.
First: the bleeding that cannot wait
Bleeding heavy enough to soak through a pad or tampon every hour for two hours or more meets the threshold ACOG gives for urgent care, especially alongside dizziness, breathlessness, or a racing heart. Most questions about heavy perimenopausal bleeding can wait until Monday. These cannot.
Dr. Nanette Santoro, a reproductive endocrinologist who has spent her career on this, describes flooding plainly: bleeding heavy enough to soak through a pad every couple of hours, over and over. That is the line. Not “a lot.” Not “worse than usual.” A rate, and a clock.
“I am bleeding through ultra-tampons in less than 2 hours to the point where they are completely saturated, and I am bleeding beyond backup pads into my clothing.”
We put that here for one reason. If you read it and felt something loosen in your chest — that is the point. This has a name, it has a definition, and it happened to a woman with a name and an age and a job who also wondered if she was making too much of it. She wasn’t. Neither are you.
Go to urgent care or the ER today if:
- You soak a pad or tampon every hour for 2 or more hours in a row
- You feel dizzy, faint, or breathless, or your heart is pounding
- You feel like you might pass out
- You are bleeding heavily and pregnancy is possible
Get an appointment this week if:
- The bleeding is very heavy or lasts more than 7 days
- It is clearly different from your normal pattern
- You are bleeding between periods or after sex
- There is real pelvic pain with it
- You are exhausted, breathless on stairs, or your heart races
- It started or got worse after you began or changed HRT
The rest of this page is for the woman whose bleeding is bad but stable. If you are in the first list, close this tab and go.
Why do periods get heavier in perimenopause?
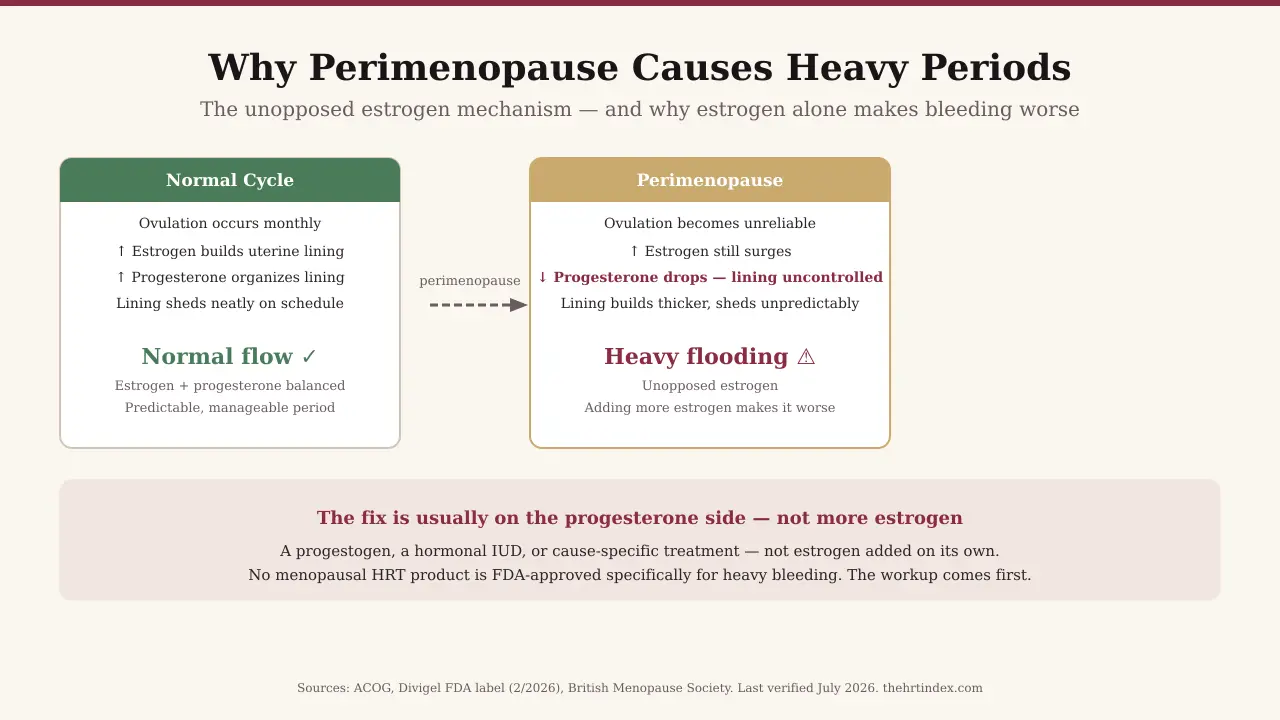
In perimenopause, ovulation becomes unreliable. In cycles where you do not ovulate, your body makes little or no progesterone — while estrogen keeps being produced, often in erratic surges. Estrogen builds the uterine lining; progesterone keeps it organized. With less progesterone to balance it, the lining can build up thicker and then shed heavily and unpredictably. That is one of the most common reasons perimenopausal periods turn heavy — though it is not the only one.
For thirty years, your ovary released an egg each month. The spot it left behind made progesterone. In perimenopause, the egg stops showing up reliably. In the cycles where it does not, there is little progesterone to do the organizing — but estrogen keeps going, and often surges harder than before. The lining gets thicker than it should, and when it finally comes away, there is more of it, sometimes all at once.
Doctors call this unopposed estrogen— estrogen without enough progesterone to balance it.
If the problem is too much estrogen relative to progesterone, then adding more estrogen alone works the wrong side of the equation. That is exactly why — when hormones are the answer — the fix is usually the progesterone side: a progestogen, or a hormonal IUD. Not estrogen by itself.
It is not always just hormones
Doctors use a framework called PALM-COEIN to sort out why any woman is bleeding abnormally. It splits causes into two groups: things you can see on a scan, and things you cannot.
| PALM — things you can see | COEIN — things you cannot |
|---|---|
| Polyp — a small growth in the lining | Coagulopathy — a bleeding or clotting disorder |
| Adenomyosis — lining tissue growing into the muscle wall | Ovulatory dysfunction — the story above |
| Leiomyoma — fibroids | Endometrial — a problem with the lining itself |
| Malignancy — cancer or pre-cancer | Iatrogenic — caused by a medication |
| Not otherwise classified |
Two causes are worth knowing about, because they show up in midlife and are easy to overlook:
- Adenomyosis— lining tissue that has grown into the muscle wall of the uterus. It causes heavy bleeding and deep, dragging pain, and it does not show up on the exam table. It needs imaging to find.
- Polyps— small growths in the lining. Usually benign, easy to remove, and no hormone will make one disappear.
- An inherited bleeding disorderlike von Willebrand disease — worth considering when heavy periods have been with you since your very first periods, or when there is a personal or family history of easy bruising and bleeding.
How heavy is “too heavy”?
In practice, heavy menstrual bleeding is defined by impact: soaking a pad or tampon every one to two hours, bleeding more than 7 days, passing clots the size of a quarter or larger, or flow that limits what you can do. If it is changing how you live, it counts.
The American Society of Hematology has flagged two things. Counting pads and tampons is an unreliable way to measure blood loss and contributes to underdiagnosis. And women judge their own bleeding against their mothers’ and sisters’ bleeding. If your mother flooded, flooding is just “what periods are” in your family. You have been using a broken ruler your whole life. That is a measurement problem, not a personal failing.
It counts as clinically heavy if any of these are true:
- You soak through a pad or tampon every 1 to 2 hours
- You need to double up — a tampon and a pad
- You get up at night to change
- You bleed more than 7 days
- You pass clots the size of a quarter or larger
- You plan your clothes, your commute, or your calendar around your period
- You have been caught out in public
The Flow Log
We built a free tool to track two cycles. You log what you used, how soaked it got, and clot size. It gives you back:
- An estimate, not a verdict— using a pictorial blood-loss scoring approach, the kind clinicians use in studies, to turn “it is really heavy” into a number you can show someone.
- A one-page printoutfor your appointment — your pattern, your estimate, and the tests worth asking for, with ferritin listed separately from a standard blood count and why.
- A safety prompt you cannot scroll past— if you log the urgent-care picture, the tool stops and points you to urgent care.
A written estimate travels better than a feeling. Remember what ASH said about pad counts getting dismissed.
Is heavy perimenopausal bleeding a sign of cancer?
Rarely — and you may have been reading the wrong number. In a 2017 systematic review of premenopausal women with abnormal bleeding, the pooled estimate for endometrial cancer among those with heavy menstrual bleeding was about 0.11% — roughly 1 in 900, and lower than for bleeding between periods. It is still worth checking if you are over 45.
| Bleeding pattern | Pooled endometrial-cancer estimate |
|---|---|
| Heavy menstrual bleeding | ~0.11% — about 1 in 900 |
| Bleeding between periods | ~0.52% — about 1 in 190 |
Heavy bleeding — the thing that scares women most, because there is so much of it — carried a lower pooled estimate than bleeding betweenperiods. The one women tend to shrug off as “just spotting” carries the higher number.
So why does everyone act like it is cancer?
The scary statistic you keep seeing — around 10% — is for postmenopausal bleeding, women who finished menopause and then started bleeding again. Completely different population, completely different risk. If you are still having periods, that is not your number.
Then why check at all?
Because 0.11% is not zero — and the math is easy once someone hands you the actual numbers. An office biopsy is quick, done in a normal exam room. Endometrial cancer caught early is one of the most curable cancers there is. ACOG recommends endometrial sampling as a first-line test for abnormal bleeding in women over 45. You are in the age band where that guidance applies.
What the February 2026 FDA change actually did — and did not do
In February 2026, the FDA approved removal of specified breast-cancer, cardiovascular, and dementia statements from the boxed warnings of an initial group of menopausal hormone therapy products. On the labels we read, “abnormal genital bleeding of unknown etiology” is still listed as the first contraindication — the door opened, but not for unexplained bleeding.
On February 12, 2026, the FDA announced the first batch of relabeled menopausal hormone therapy products. The boxed warning got cut back. That is real, and it is a genuinely big shift.
But we went and read one of the actual labels — not the press release. Divigel (estradiol gel), revised 2/2026, Reference ID 5744952. Every FDA label opens with a box called RECENT MAJOR CHANGESlisting what was touched. Divigel’s includes both of these lines:
Boxed Warning, Cardiovascular Disorders, Breast Cancer, Probable Dementia — removed 2/2026
Contraindications (4) — 2/2026
The contraindications section was revised in the same February update. Here is what it still says:
4 CONTRAINDICATIONS
Divigel is contraindicated in women with any of the following conditions:
• Abnormal genital bleeding of unknown etiology
• Current or history of breast cancer…
First on the list. (“Of unknown etiology” means nobody has worked out the cause yet.)
The trial data on the same label
Divigel’s label reports side effects from its pivotal trial (495 women). Here is the row that matters:
| Adverse reaction | Divigel 0.25 g | Divigel 0.5 g | Divigel 1.0 g | Placebo |
|---|---|---|---|---|
| Metrorrhagia (irregular uterine bleeding) | 4.1% | 5.7% | 9.6% | 1.6% |
At the highest dose, irregular bleeding was reported in 9.6% of women versus 1.6% on placebo. Estrogen is not a bleeding treatment. For this drug, in its own trial, bleeding was a side effect of it.
Undiagnosed abnormal bleeding is a contraindication in current systemic-estrogen labeling like Divigel’s. That means the cause needs to be found before that product is started — not that HRT is off the table forever. Not a door slammed. A sequence. And the sequence is printed on the drug.
The useful question is not “am I on the relabeled list.” It is “what does my manufacturer’s current label say?”We checked two estradiol gel generics — from Amneal and Padagis — and both logged the same 2/2026 removals with contraindications revised the same month. The Divigel label is public.
Why does the advice you are reading feel slightly off? It is probably British
Many of the pages ranking for this question are UK sources, and UK hormone licensing differs from US FDA approval in ways that matter here. In Britain, the Mirena IUD is licensed as the progestogen half of HRT; in the US that exact use is off-label. Sequential HRT is standard NHS practice; no US menopausal HRT product carries an approval for cycle regulation.
Have you noticed the advice you are finding is confident, well-written, and somehow describing a healthcare system you do not quite live in? You are not imagining it. “Off-label” means a drug is being used for something the FDA has not formally approved. It is legal and common; doctors do it every day. But it changes what your insurance may cover, and it changes how a conversation goes when you ask for something by name.
| What UK pages tell you | UK status | US status | What it means for you |
|---|---|---|---|
| Use a Mirena as the progestogen part of your HRT | Licensed — ~4-year licence for endometrial protection within HRT | Off-label. Mirena’s FDA approvals are contraception and heavy menstrual bleeding, not endometrial protection alongside estrogen | Legal and common, but off-label. Coverage varies by plan |
| Take sequential HRT to make your periods predictable | Standard NHS practice; licensed products available | No FDA-approved menopausal HRT product is approved for cycle regulation | Good to know before you ask for it by name |
| The hormonal IUD controls heavy periods | Licensed | FDA-approved — with a condition attached (see next section) | True, and often the best option — but the condition matters |
| Tranexamic acid for heavy periods | Licensed | FDA-approved (Lysteda) — for cyclic heavy bleeding; label says rule out lining problem first | Two catches nobody mentions — both coming up below |
This is not a knock on British medicine. The advice that has been confusing you was written for a different regulator. You were not failing to understand it — it genuinely did not apply to you.
Why you are exhausted when your blood test came back “normal”
A normal blood count does not mean your iron is fine. A standard blood count (CBC) measures hemoglobin — the iron moving through your blood right now. Ferritin measures stored iron, and stores empty long before hemoglobin drops. A normal CBC cannot rule out iron deficiency, and the symptoms of low iron overlap almost exactly with what many women blame on perimenopause.
This is the section we would keep if we had to delete every other one.
When you bleed heavily month after month, your body does not drain the checking account first. It quietly drains the savings — your stored iron (ferritin) — to keep the circulating iron (hemoglobin) looking full. So your CBC comes back “normal” while your stores run low. In a cohort of 362 women with bleeding disorders, 41.7% had normal hemoglobin and were iron deficient once someone actually checked their iron studies (ASH, 2025). That is proof that normal hemoglobin can hide iron deficiency.
| Symptoms of iron deficiency without anemia | Symptoms often blamed on perimenopause |
|---|---|
| Fatigue that sleep does not fix | Fatigue that sleep does not fix |
| Brain fog | Brain fog |
| Hair shedding | Hair shedding |
| Breathless on stairs | Breathless on stairs |
| Poor exercise tolerance | Poor exercise tolerance |
| Restless legs | (you did not know that one was on the list) |
The American Society of Hematology, in its own publication (March 2025), stated that clinicians do not believe women who report heavy vaginal blood loss and “serially disregard their symptoms, resulting in health care-related trauma that further blocks the opportunity for diagnosis and treatment.” We cannot give you back the time spent being brushed off. But we can hand you that citation.
The lab you will be offered vs. the one worth asking for
You may be offered a hormone panel — FSH, estradiol. The Divigel label says in writing (Section 5.20): “Serum follicle stimulating hormone (FSH) and estradiol levels are not useful in the management of moderate to severe vasomotor symptoms.” Meanwhile, the test that could explain your worst symptom often goes unordered.
If you have heavy bleeding plus symptoms from that table, ask specifically:
“Can we check a ferritin, not just a CBC?”
A CBC is the default order. Ferritin is a separate box someone has to tick on purpose. When the result comes back, ask for the actual number — not just “normal.” Ranges vary, and a number near the bottom of the range can still explain how you feel.
What actually stops heavy bleeding: the FDA-labeled options
Several products are FDA-labeled for heavy menstrual bleeding — but they do not all treat the same cause. Which one fits you depends entirely on why you are bleeding. There is no FDA-approved treatment for “heavy bleeding, cause unknown.”
| Treatment | FDA-labeled for heavy bleeding? | What the label actually covers | The catch |
|---|---|---|---|
| Mirena / Liletta (52 mg hormonal IUD) | Yes — up to 5 years | Heavy bleeding “for women who choose to use intrauterine contraception as their method of contraception” | Approval is tied to wanting contraception |
| Lysteda (tranexamic acid) | Yes | Treatment of cyclic heavy menstrual bleeding; label says exclude endometrial pathology first | Taken only during your period (up to 5 days). Contraindicated with combined hormonal birth control — a clotting-risk issue |
| Natazia (estradiol valerate / dienogest) | Yes — the only birth control pill that is | Heavy bleeding “not caused by any diagnosed conditions of the uterus… in women who decide to use the Pill for birth control” | Two conditions at once: you want the Pill for birth control, and a uterine cause has been ruled out |
| Myfembree / Oriahnn (GnRH combos) | Yes — for fibroid-related bleeding | Heavy bleeding associated with uterine fibroids in premenopausal women | Only if fibroids are the cause. Limited to ~24 months due to bone-loss risk |
| Meclofenamate (NSAID) | Has specific labeling | Labeling related to excessive menstrual blood loss; product-specific | Not every NSAID carries this; product and label matter |
Look at the “what the label covers” column. Some options are gated on wanting contraception. One is gated on ruling out a uterine cause. Two only apply if fibroids are the reason. Every single approved path assumes someone already knows why you are bleeding. That is the reason the workup is step one — and it is printed on the labels, not invented by us.
“It gets worse before it gets better” — the Mirena thing nobody warns you about
If you get a hormonal IUD, bleeding and spotting often increasein the first months after insertion, and it can take several cycles for the benefit to show. Guidance suggests giving it at least six months. When nobody says that: she gets the IUD hoping for relief, bleeds more at week six, and has it removed at week eight — quitting the treatment during the exact window where it looks like it is failing. Mark six months on your calendar and judge it then. Contact your clinician sooner for severe bleeding, significant pain, fever, or signs the device has moved.
Options used off-label
- Cyclic oral progestogens— used for bleeding control. The FDA-labeled indication depends on the exact product; “progesterone” is not one interchangeable drug.
- Most combined birth control pills— used for cycle control. Natazia is the only one FDA-approved for heavy bleeding; the rest are off-label for it.
- Ibuprofen and similar NSAIDs— can reduce flow somewhat; used off-label for this. (Meclofenamate is the one with specific labeling, above.)
Off-label does not mean bad. It means you should know which one you are being offered, and be able to ask why.
HRT, the pill, or progesterone? What each one is actually for
Menopausal HRT mainly treats hot flashes and night sweats. Hormonal birth control suppresses ovulation and prevents pregnancy while controlling the cycle. “Progesterone” refers to several different drugs doing several different jobs. They are not interchangeable, and menopausal HRT does not prevent pregnancy.
Four medicines, four jobs. This is the table we wish someone had handed you two years ago.
| Menopausal HRT | Combined birth control pill | 52 mg hormonal IUD | Oral progesterone / progestin | |
|---|---|---|---|---|
| Main job | Treat hot flashes and night sweats | Suppress ovulation, control cycles, prevent pregnancy | Reduce heavy bleeding + prevent pregnancy | Depends entirely on the product |
| Prevents pregnancy? | No | Yes | Yes | Not necessarily |
| FDA-approved for heavy bleeding? | No (menopausal products) | Only Natazia | Yes (with the condition) | Depends on the product |
| Treats hot flashes? | Yes — that is the approval | May help some women; it is not menopausal HRT | No | Usually not on its own |
| Needs a procedure? | No | No | Yes | No |
Why “progesterone” causes so much confusion
- Progesterone (the natural molecule) and progestins (synthetic versions) are not the same drug.
- It can be delivered by mouth, by IUD, or inside a combination product. Route changes everything.
- It can be doing any of three different jobs: protecting your lining while you are on estrogen, preventing pregnancy, or reducing bleeding.
When someone says “you need progesterone,” that sentence has not told you much yet. The question to ask, word for word:
“Is this being used to treat my bleeding, to protect my lining while I am on estrogen, to prevent pregnancy, or more than one of those?”
Do you still need birth control? It changes your options
Pregnancy remains possible throughout perimenopause, and menopausal HRT is not contraception. This matters beyond pregnancy: two of the FDA-approved treatments for heavy menstrual bleeding are approved specifically for women choosing that method as contraception. So whether you still want birth control genuinely shapes which approved treatments fit.
Look again at the label wording from the treatment table. Mirena: “for women who choose to use intrauterine contraception as their method of contraception.” Natazia: “in women who decide to use the Pill for birth control.” For those products, contraception is part of the labeled treatment context. It cuts both ways: if you have decided you are past needing birth control, some of these options may be a poorer fit.
Menopausal HRT does not prevent pregnancy. It is not contraception and was never designed as it. If you are on HRT, still having any periods, and do not want to be pregnant, HRT is not covering you.
- You want bleeding control and birth control: the hormonal IUD or Natazia are aimed at both. Often the strongest position to be in.
- You are sure you do not need birth control: tranexamic acid is a nonhormonal option; cause-specific treatment is the other route.
- You are not sure: that is a real conversation with a clinician, and since it changes your options, have it before you settle on a treatment.
What a correct workup looks like — and what it costs
For heavy bleeding over 45 the workup commonly includes a pregnancy test if relevant, a CBC and iron studies, sometimes thyroid testing, a pelvic ultrasound when a structural cause is suspected, and endometrial sampling. ACOG recommends sampling as a first-line test for abnormal bleeding over 45. Where you get each test can change the price dramatically.
The pieces a clinician may use:
- Pregnancy test, if pregnancy is possible
- CBC and ferritin— ask for both
- Thyroid testing, if symptoms point that way
- Transvaginal ultrasound— when fibroids, polyps, or adenomyosis are suspected
- Endometrial biopsy— ACOG recommends it for abnormal bleeding over 45, and for younger women with risk factors
- Saline sonohysterography or hysteroscopy— when a lining lesion is suspected or the ultrasound leaves questions
The Code Card
Every test has a billing code. Call and ask “how much is an ultrasound” and you will get transferred twice and told they cannot say. Ask for the cash price for CPT 76830, and you will often get a number.
| What you want | The code to ask for |
|---|---|
| Transvaginal ultrasound (non-obstetric) | CPT 76830 |
| Endometrial biopsy, in-office, no cervical dilation | CPT 58100 |
| Item | Reported self-pay range | What to know |
|---|---|---|
| Transvaginal ultrasound (CPT 76830) | roughly $250–$600 | The identical scan billed through a hospital outpatient department can run far higher. Freestanding imaging centers tend to be dramatically cheaper |
| Endometrial biopsy (CPT 58100) | Medicare reimburses ~$100; self-pay charges vary | Call and ask by code rather than trusting any one number. Ask whether the quote includes the pathology fee |
“Does the biopsy hurt?”
You want to know and you are not going to ask. So here is the honest version. It is usually a brief in-office procedure — no operating room. Most women describe intense cramping, similar to a bad period cramp, for around 30 to 60 seconds, and then it is done. Taking ibuprofen an hour beforehand genuinely helps, and it is worth asking what pain relief they offer. But we are not going to tell you it is nothing — you would find out, and stop trusting the rest of this page. It is a short, sharp cramp to close out a real question. That is the actual trade.
Where online care fits — and where it does not
Telehealth can take a proper history, order labs including ferritin, and tell you whether you likely need imaging. It cannot perform a pelvic exam, an ultrasound, or a biopsy. For heavy bleeding, the sequence that fits most stable women is virtual for the history and labs, in person for anything involving a probe — and in-person first when the bleeding pattern points to a scan or procedure.
Everything above this line was free, with nothing to buy in it. That was deliberate. Now we will tell you where online care earns its place and where it does not — and you can judge whether we have been straight with you.
Read your provider’s own words
| Where | What Midi says | Which kind of care |
|---|---|---|
| joinmidi.com/how-midi-works | “In-person exams reveal very little that you can’t tell us yourself. In fact, after age 45, the only routine in-person Ob/Gyn care you need is a Pap smear…” | Routine |
| Midi’s own article on heavy periods after 40 (Jan 2026) | “ongoing heavy periods after age 40 shouldn’t be dismissed, even if initial exams or blood work come back normal… Even virtual clinics, like Midi, can refer you for in-person care to get necessary screening tests.” | Symptomatic |
Those two statements do not contradict each other — the difference between them is the most useful thing on this page. The first is true for routine care. Heavy bleeding is not routine care. Midi’s own clinical writing says so, plainly, in its own words.
The honest version, if we were not selling anything:
Midi cannot perform the two things you may most need. No transvaginal ultrasound, no endometrial biopsy — not during a virtual visit. Its clinicians can order labs and refer you for local in-person testing, but the scan or procedure itself happens elsewhere. If the thing standing between you and an answer is imaging, Midi is not your first call this week.
→ If you need the scan, skip to Sesame below — cash-pay in-person gynecology and pelvic ultrasounds, no insurance required.
But here is what a virtual visit actually buys you. Midi operates in all 50 states and states it works with many PPO plans. Its clinicians can order the CBC and ferritin nobody has ordered you, take the structured history that helps sort which PALM-COEIN cause you are dealing with, and tell you whether you need the ultrasound at all. Getting the right test ordered — by someone who takes you seriously — is the bottleneck. That is the part a good virtual visit is genuinely good at.
Midi’s limits, stated plainly:
- Medicare:you can be seen, but as self-pay only — claims cannot be submitted.
- Medicaid: not accepted. Here is the coverage path instead
- Coverage depends on your plan and state; deductibles and copays still apply.
- Midi offers a compounded line. Compounded drugs are not FDA-approved — that is the FDA’s position generally. Walk in and ask which options are FDA-approved for your situation, and whether anything suggested is compounded or off-label.
Sesame — the in-person bridge
Sesame is a cash-pay marketplace: you pick a clinician, see the price up front, and book. You may need a scan and an in-person exam, and that is not a telehealth product. Where Sesame lists local in-person gynecology or pelvic imaging, it shows upfront cash pricing by location. Sesame advertises some visits starting around $34 — but that is for general visits; gynecology and imaging prices depend on what is listed near you, so check your ZIP before assuming.
One thing to check yourself: Sesame Plus includes some free labs — CBC, CMP, HbA1c are listed. We have not been able to confirm ferritin is included, and for this page ferritin is the point. Confirm it is covered before you pay.
And if you are actively flooding right now, do not start with either of them. Urgent care or your OB/GYN’s on-call line, today. Telehealth is for the woman whose bleeding is bad but stable and who needs the right workup started — not for a bleeding emergency.
If you have hot flashes too: the sequencing question
Many women in perimenopause have both heavy bleeding and hot flashes, and the good news is you usually do not have to choose. ACOG says hormone therapy can help perimenopausal heavy bleeding and hot flashes together — but unexplained bleeding gets evaluated before systemic estrogen starts. Sort the cause first; then a clinician can often treat both.
We have spent this page telling you estrogen is not the answer to your bleeding on its own. So let us be clear about what we are notsaying. We are not saying HRT is not for you. If you are waking up soaked at 3am, having hot flashes in meetings, not sleeping — those are real and treatable, and systemic estrogen is good at treating them.
The sequence usually runs like this:
- Find out why you are bleeding. Labs, a scan if needed, a biopsy if you are over 45.
- Treat the bleeding with something suited to the cause.
- Handle the hot flashes— often in the same plan, once the bleeding is understood.
The word doing the work in that contraindication is unknown. Finding the cause removes the main barrier.
Two things worth knowing before that conversation:
- The elegant option, honestly labeled. The 52 mg hormonal IUD can treat heavy bleeding (FDA-approved, with the contraception condition) andserve as the progestogen alongside estrogen for hot flashes — one device covering both the bleeding and the lining protection while estrogen handles the flashes. In the US, that second use is off-label. Legal, common, often excellent — just know which part is approved and which is not, because your insurer will.
- What might be said to you.If someone suggests you are “too young” for HRT, the estradiol gel label’s own timing language notes that starting HRT is generally considered in women under 60 or within 10 years of menopause. That is about timing, not a hard eligibility rule.
Read next: HRT benefits and risks · Non-hormonal options · What HRT costs in 2026
What we actually verified
What we checked for this page, and when
- ACOG guidance— confirmed ACOG states hormone therapy can be helpful for heavy menstrual bleeding during perimenopause, and that periods are often lighter and more predictable on it. Verified July 2026.
- Divigel FDA label, revised 2/2026(Reference ID 5744952) — read the full prescribing information; confirmed the February 2026 revision kept “abnormal genital bleeding of unknown etiology” as the first contraindication, and reported the metrorrhagia figures in its trial table. Verified July 2026.
- Two estradiol gel generics(Amneal, Padagis) — confirmed both logged the same 2/2026 removals with contraindications revised the same month. Verified July 2026.
- Mirena, Lysteda, and Natazia labeling— confirmed each heavy-bleeding indication and its conditions, including that Lysteda is contraindicated with combined hormonal contraceptives. Verified July 2026.
- Myfembree and Oriahnn— confirmed FDA approval for heavy menstrual bleeding associated with uterine fibroids in premenopausal women. Verified July 2026.
- Pennant et al., BJOG 2017;124:404–411— the pooled ~0.11% and ~0.52% estimates, from 29,059 premenopausal women.
- British Menopause Society— confirmed the UK licence for the LNG-IUS for endometrial protection within HRT, and that no equivalent FDA indication exists.
- Midi Health and Sesame Care— quoted directly from their own published pages (provider-stated). Verified July 2026.
- CPT 76830 and CPT 58100— confirmed as the correct billing codes. Verified July 2026.
What we did not do:We did not sign up with any provider, place an IUD, undergo a biopsy, or test a cancellation flow. We could not confirm a reliable national cash price for an endometrial biopsy from a primary source, or whether Sesame Plus’s lab benefit includes ferritin — and we have said so rather than guess. Provider claims are labeled provider-stated; we did not independently verify appointment wait times or local availability everywhere.
This page is editorial research. It has not been reviewed by a clinician. It is not medical advice. Our medical review policy. How we work: The HRT Index Verification Standard · Corrections
By The HRT Index Editorial Team · About our team
Frequently asked questions
- Does HRT stop heavy periods?
- It can help, but not on its own — estrogen alone can make heavy bleeding worse. ACOG says hormone therapy can help heavy perimenopausal bleeding, usually through the progestogen side or a hormonal IUD. No menopausal HRT product is FDA-approved specifically for heavy bleeding, and unexplained bleeding needs a workup first.
- Can HRT make heavy bleeding worse?
- Yes. Adding estrogen without enough progestogen can thicken the lining and increase bleeding, and unscheduled bleeding is a common side effect in estrogen trials. If bleeding starts or worsens after you begin or change HRT, call your prescriber rather than waiting it out.
- What if I'm already on HRT and start bleeding heavily?
- Contact your prescriber. Some spotting can be expected early on or after a dose change, and sequential regimens include a planned monthly bleed — but heavy, prolonged, or new bleeding after a stable stretch should be reviewed, especially if it has been more than 12 months since a natural period. Do not adjust your estrogen or progestogen on your own.
- What is the difference between sequential and continuous HRT for bleeding?
- Sequential (cyclical) HRT adds a progestogen for part of each month and usually produces a planned monthly bleed — often used closer to perimenopause. Continuous-combined HRT gives both hormones daily and is generally designed to avoid regular bleeding, typically for later use. Which fits depends on where you are relative to menopause; it is a clinician's call, not a self-adjustment.
- What is the fastest way to reduce heavy perimenopausal bleeding?
- Tranexamic acid (Lysteda) works during your period and is FDA-approved for cyclic heavy bleeding. The 52 mg hormonal IUD works over months and is approved for up to five years. Both require ruling out a cause first — Lysteda's label says so in its indications.
- Why am I so exhausted if my blood test was normal?
- A standard blood count measures hemoglobin, not stored iron, so it can miss iron deficiency. Ask for a ferritin — a separate test that has to be ordered on purpose — especially if you have fatigue, brain fog, hair shedding, or breathlessness alongside heavy bleeding.
- Is heavy bleeding in perimenopause a sign of cancer?
- Rarely. In premenopausal women with heavy menstrual bleeding, the pooled endometrial-cancer estimate was about 0.11% — roughly 1 in 900, and lower than for bleeding between periods. It is still worth checking if you are over 45, because the test is quick and the disease is very curable when caught early.
- Do I need an endometrial biopsy?
- ACOG recommends endometrial sampling as a first-line test for abnormal uterine bleeding in women over 45, and for younger women with risk factors or persistent bleeding. It is an in-office procedure — usually a short, sharp cramp, no operating room.
- Can I get treated for heavy periods online?
- Partly. Telehealth can take a history, order labs including ferritin, and tell you whether you likely need imaging. It cannot perform an ultrasound or a biopsy. For heavy bleeding, virtual care is often the fastest way to get the right test ordered — but the test itself happens in person.
- How long do heavy perimenopausal periods last?
- Bleeding driven by erratic ovulation often eases as your cycles end. But fibroids, polyps, adenomyosis, medication effects, and lining conditions follow their own course and do not necessarily resolve at menopause. Persistent or recurrent bleeding — especially after 12 months without a period — needs evaluation.
- Will I need a hysterectomy?
- Many women are treated without one. Whether you need it depends on the cause, the severity, your fertility goals, and how you respond to medication or a hormonal IUD. Surgery is generally considered after other options, not first.
- Can I use a Mirena as part of HRT?
- In the UK it is licensed for that. In the US that use is off-label — legal and common, but not an FDA-approved indication, so your insurer may treat it differently for that purpose.
- Does HRT prevent pregnancy?
- No. Menopausal HRT is not contraception, and pregnancy remains possible during perimenopause because ovulation becomes unpredictable rather than stopping outright.
- Can I take tranexamic acid while on HRT?
- Tranexamic acid is contraindicated with combined hormonal birth control because of clotting risk. Menopausal HRT is a different category, so whether they can be combined depends on your exact estrogen or progestogen product, your clotting history, and other risk factors — a decision for your prescriber or pharmacist, not a blanket yes or no.