The quick answer, by situation
Find your row. The rest of the page explains each one.
| Your situation | The bottom line |
|---|---|
| Uterus + systemic estrogen alone (no progestogen) | The clearest higher-risk setup. Confirm what's protecting your lining. |
| Uterus + estrogen plus a progestogen (combined HRT) | Generally protective when it's dosed and taken as prescribed. |
| Low-dose vaginal estrogen (like Estring) | A different, lower-risk category. Still report any bleeding. |
| No uterus (confirmed total hysterectomy) | This risk mostly doesn't apply — but confirm your surgery type. |
| Compounded "bioidentical" progesterone cream | Protection isn't established. This is the one to scrutinize. |
| Bleeding after menopause | See a clinician promptly. A table can't tell you the cause. |
This guide is for you if
- You take or are considering menopause HRT and still have a uterus
- You’re not sure why you need progesterone — or whether you do
- You want to know if a patch, pill, gel, or vaginal cream changes the answer
- You saw a scary post or news story and want the real picture
- You want to walk into your appointment knowing what to check
Don’t rely on this page alone if
- You’re bleeding after menopause, or bleeding heavily or often
- You’ve had endometrial hyperplasia, atypical hyperplasia/EIN, or endometrial cancer
- You don’t know what kind of hysterectomy you had, or you’ve had an endometrial ablation
- You’re thinking about stopping your progesterone because of side effects
- You have a pending or abnormal ultrasound or biopsy
Not sure which row is yours? Our free matching tool maps your symptoms, anatomy, and route preference to the right starting point in about 90 seconds — and tells you honestly when you should see someone in person first.
See which care path fits your situation →Heads up: Find My HRT Path may show telehealth providers we have an affiliate relationship with. If you start care through one, we may earn a commission — at no extra cost to you, and it never changes what this page tells you.
HRT and endometrial cancer risk: what actually drives it
Some HRT raises endometrial cancer risk and some doesn’t — it comes down to the regimen. The clearest higher-risk setup is systemic estrogen with no progestogen when you still have a uterus. Current U.S. estrogen labeling reports that women using unopposed systemic estrogen who have a uterus have an endometrial cancer risk about 2 to 12 times higher than non-users, rising to roughly 15 to 24 times higher after five to ten or more years of use. Add adequate protection and that excess risk largely disappears. [1][2]
The endometrium is the lining inside your uterus — the tissue that used to build up and shed each month before menopause. Estrogen tells that lining to grow. Progesterone (and its lab-made cousins, called progestins — together the whole family is called progestogens) tells it to stop and settle down. That balance is the entire safety story.
Take estrogen alone, with a uterus, and the lining keeps getting the “grow” signal with no “stop.” Over time that can lead to overgrowth (hyperplasia) and, in some cases, cancer. [1][2] The risk climbs the longer unopposed estrogen is used — it can even linger for years after stopping. [2]
The honest part
We can’t calculate your personal risk, and “I’m on combined HRT” is not, by itself, a complete safety description. Your exact estrogen, your exact progestogen, the dose, the schedule, how reliably you take it, your anatomy, and your history all change the answer.
The reassuring part
You don’t need us to calculate your risk. You need to know what to check — and that’s a short, doable list. The risk is conditional. The conditions are knowable. And for almost every situation, there’s a clear next step.
Do I need endometrial protection after hysterectomy?
If you don’t have a uterus, there’s no endometrium to protect, so the unopposed-estrogen risk mostly doesn’t apply — and a progestogen usually isn’t needed. If you do have a uterus and use systemic estrogen, you need protection. This single fact reorganizes the whole conversation.
"I had a hysterectomy" isn't always the full story
A total hysterectomy removes the uterus and its lining. But a supracervical (partial) hysterectomy leaves the cervix — and sometimes a small amount of tissue — behind. If you're not 100% sure what was removed, don't lean on the "no uterus = no protection needed" rule until you've confirmed it.
An endometrial ablation is not a hysterectomy
Ablation treats the lining but doesn't remove the uterus, and some endometrial tissue can remain. So if you've had an ablation and use systemic estrogen, you still need a clinician-directed protection plan — U.K. menopause guidance specifically recommends combined HRT for women who use HRT after an ablation. [3]
How to confirm
Ask for your operative report or pathology report, or ask the clinician who manages your care. It's a concrete question that settles a big one.
Which HRT setups raise, lower, or leave endometrial cancer risk uncertain?
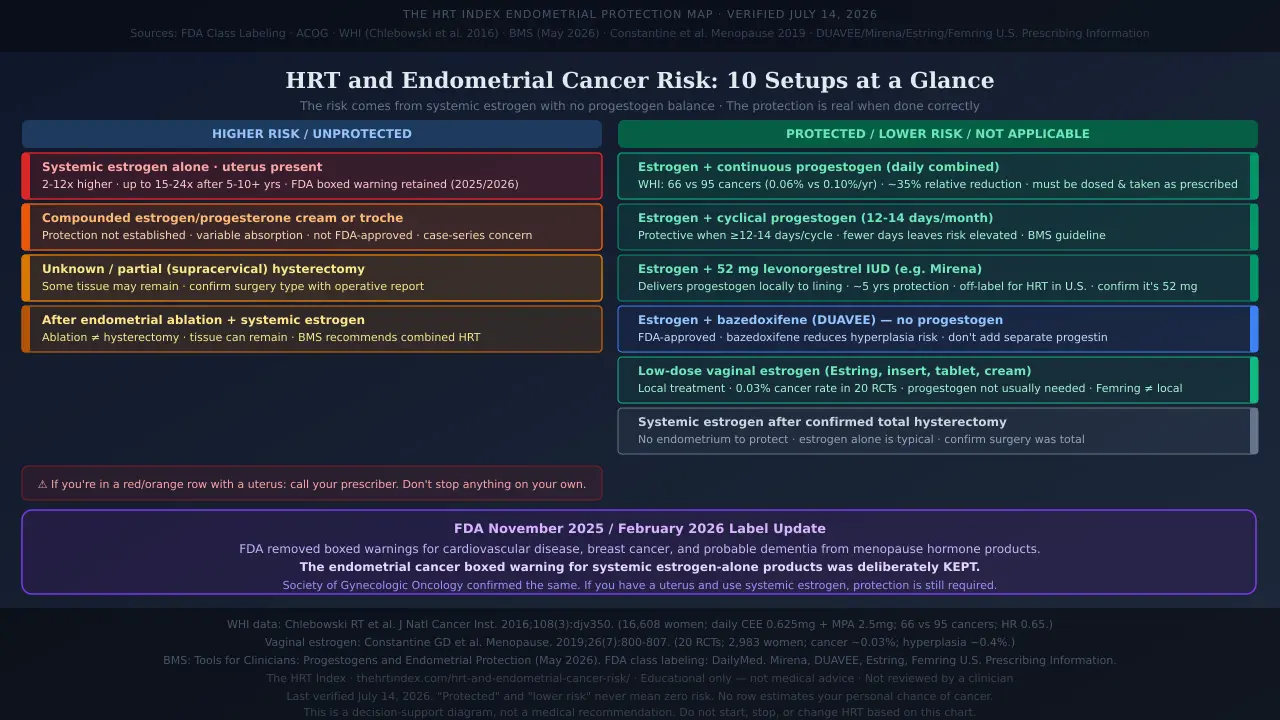
The clearest higher-risk setup is systemic estrogen with no protection when you have a uterus. Combined regimens, a hormonal IUD, a progestogen-free combination, low-dose vaginal estrogen, no uterus, and compounded products are all different situations — they are not interchangeable. We assembled these U.S.-relevant setups from current FDA labels, clinical guidance, and peer-reviewed evidence.
| Your HRT setup | Protects the lining? | What the evidence says | U.S. regulatory status | What to check |
|---|---|---|---|---|
| Systemic estrogen alone (pill, patch, gel, spray) with a uterus | No — this is the risk | Reported endometrial cancer risk about 2–12× non-users; up to 15–24× after 5–10+ years; can linger years after stopping. [2] | FDA-approved products exist; estrogen-alone use with a uterus carries an endometrial-cancer boxed warning kept by FDA in 2025. | Call your prescriber — what protects your lining? |
| Estrogen + continuous progestogen (daily combined) | Yes — when dosed and taken as prescribed | WHI trial of daily CEE 0.625 mg + MPA 2.5 mg: 66 vs 95 cancers (0.06% vs 0.10%/yr); ~35% relative reduction. Evidence is regimen-specific. [4] | FDA-approved fixed combinations (e.g., Bijuva). Separately prescribed products keep own approvals. | Exact progestogen, dose, schedule; consistency of use |
| Estrogen + cyclical/sequential progestogen (part of the month) | Yes — with enough progestogen days | Protective when the progestogen runs long enough; too few days leaves risk elevated; very long-term cyclical use is less certain. U.K. guidance: 12–14 days/month. [3] | May use FDA-approved products; assembled cyclic schedule may be off-label. | How many days/month; how long you’ve used it |
| Estrogen + 52 mg levonorgestrel IUD (e.g., Mirena) | Yes | The 52 mg levonorgestrel IUD delivers progestogen right to the lining; supports endometrial protection for up to ~5 years within HRT. [3] | FDA-approved for contraception and heavy periods. Using it as the progestogen part of menopausal HRT is off-label in the U.S. [5] | That it’s the 52 mg type; insertion and replacement dates |
| Estrogen + bazedoxifene (DUAVEE) — no separate progestogen | Yes — no separate progestogen | Per its label, the bazedoxifene component reduces the risk of endometrial hyperplasia that can occur with the estrogen component. [6] | FDA-approved for women with a uterus (hot flashes; osteoporosis prevention). | Don’t add another estrogen or progestin without prescriber’s guidance |
| Low-dose vaginal estrogen (Estring, low-dose cream, tablet, insert) | Low lining effect; protection usually not needed | Across 20 randomized trials (2,983 women), reported cancer and hyperplasia rates were about 0.03% and 0.4%; most data ran up to a year. A progestogen generally isn’t recommended with it. [7][8] | FDA-approved low-dose local products exist. Femring is systemic, not local — different category. | Confirm your exact product; Estring is local, Femring is not; report any bleeding |
| Systemic estrogen after confirmed total hysterectomy | Not applicable — no lining | With no endometrium, this risk mostly doesn’t apply; estrogen alone is the usual approach. [9] | FDA-approved estrogen-alone products. | That your hysterectomy was total; any relevant history |
| Unknown or partial (supracervical) hysterectomy | Undetermined until confirmed | Some endometrial tissue may remain, so the “no uterus” rule can’t be assumed. | Depends on the products used. | Your operative or pathology report; clinician confirmation |
| After endometrial ablation + systemic estrogen | Protection still needed | Ablation isn’t a hysterectomy; endometrial tissue can remain. U.K. guidance recommends combined HRT for women using HRT after ablation. [3] | Depends on the products used. | Confirm the plan with a clinician; don’t assume ablation replaces protection |
| Compounded estrogen and/or progesterone (cream, troche) | Uncertain — not established | Compounded transdermal progesterone has variable absorption and may not provide adequate protection; a published case series reported endometrial cancers in women using compounded “bioidentical” HRT. [3][10] | Not FDA-approved. [11] | Exact ingredients, route, dose, pharmacy; and the protection plan |
How to read this map: find your setup, then read across. If you’re in the top row and have a uterus, that’s your cue to call your prescriber and ask what’s protecting your lining — not to stop anything on your own. Don’t start, stop, or change HRT based on a table.
Want to match your exact setup to the right next step?Answer a few quick questions and we’ll point you to the right kind of care for your anatomy, symptoms, and route — and flag when you should start with an in-person clinician.
See which care path fits your situation →Does the type of estrogen — patch, gel, pill, or spray — change whether I need protection?
No. A patch, gel, and spray are all systemicestrogen, meaning the hormone reaches your whole body — so if you have a uterus, you still need endometrial protection. “Systemic” and “oral” are not the same thing; switching from a pill to a patch changes the delivery, not the need to balance estrogen at the lining.
A patch can be a good choice for reasons that have nothing to do with your uterus — estrogen absorbed through the skin skips the first pass through the liver, and transdermal estrogen is linked to a lower risk of blood clots than pills. [12] That’s a genuine benefit. But it’s a clot benefit, not a lining benefit. A skin patch does not turn systemic estrogen into local treatment, and it does not make unopposed estrogen safe for the endometrium.
Write these down before your visit
The exact name of your estrogen, its route (pill, patch, gel, spray), its strength, how often you use it, whether it’s meant for whole-body or vaginal symptoms, and — if you have a uterus — the name and schedule of your progestogen. Then ask: “Is my estrogen systemic, and what exactly is protecting my uterine lining while I use it?”
How much does progesterone actually lower the risk?
There’s no single percentage that fits every regimen, but the direction is clear and reassuring: a progestogen counters estrogen’s effect on the lining and generally removes the excess risk of unopposed estrogen. In the Women’s Health Initiative trial of one specific daily regimen — 0.625 mg conjugated equine estrogen plus 2.5 mg medroxyprogesterone acetate — there were fewer endometrial cancers than with placebo (66 vs 95 cases; about 0.06% vs 0.10% per year). [4]
The WHI numbers in plain terms
Over a median 5.6 years of treatment and about 13 years of follow-up: roughly a 35% relative reduction, and an absolute difference of about 0.04 percentage points per year. The protective regimen didn’t just hold the line — it came out slightly below the no-hormone group.
The fine print — because it matters
- Those numbers describe one regimen in one study. They don’t prove every combination, every dose, or every product performs identically.
- How you take it counts. Repeatedly missing doses, or stopping the progestogen while continuing systemic estrogen, can reduce the protection. Ask your prescriber how to handle missed doses for your exact regimen.
- “I take progesterone” isn’t enough detail. To know whether your setup is reassuring, a clinician needs the exact medication, route, dose, whether it’s daily or cyclical, and the estrogen it’s balancing. See also: micronized progesterone side effects.
Is continuous or cyclical HRT safer for the uterus?
Continuous combined HRT — estrogen and a progestogen taken together every day — has the most direct evidence for avoiding excess endometrial risk. Cyclical (sequential) HRT, where the progestogen is taken during part of each cycle, is protective when done correctly but depends more on the exact schedule and duration.
Continuous combined
Both hormones, daily, ongoing. Usually no monthly bleed once your body settles. This is the setup with the strongest track record for the lining.
Cyclical / sequential
Estrogen daily, progestogen for part of the month. Often produces a scheduled monthly bleed, which is expected. Commonly used closer to the menopause transition.
One nuance worth knowing: with cyclical HRT, too few progestogen days a month leaves risk elevated, and using a sequential regimen beyond about five years may carry a small extra endometrial risk. [3] The questions that actually tell you whether a schedule is reassuring: What exact progestogen? How many days a month? How long have I been on it? What bleeding is expected? See also: progesterone side effects in menopause.
Is compounded “bioidentical” progesterone safe for my uterus?
This is the setup to scrutinize. Compounded progesterone — made to order by a pharmacy as a cream, troche, or lozenge — has documented concerns about whether it actually protects the endometrium. Compounded transdermal progesterone has variable absorption and may not deliver a protective dose, and a published case series reported endometrial cancers in women using compounded “bioidentical” HRT. [3][10]
- Compounded products are not FDA-approved. FDA-approved drugs go through FDA review for safety, effectiveness, quality, and manufacturing; compounded drugs generally do not get that premarket review. [11]
- The FDA does not verify their safety, effectiveness, or quality before they’re sold. [11]
- Testing of sampled compounded hormone products has found the amount of active ingredient can vary from product to product. [13]
- Major menopause societies don’t recommend compounded hormones for menopause symptoms when an FDA-approved option exists. [14]
The options with the clearest evidence for endometrial protection are FDA-approved systemic progestogens (like oral micronized progesterone or medroxyprogesterone), an FDA-approved combined product, or — used off-label in the U.S. — a 52 mg levonorgestrel IUD. [3][5]
If a compounded program is what you’re using or being offered
Don’t let the part that protects your uterus be the compounded part without asking hard questions — the exact ingredients, the route, the dose, the pharmacy, and what evidence supports the protection plan. If that conversation isn’t reassuring, that’s your signal to get a second opinion.
Does low-dose vaginal estrogen increase endometrial cancer risk?
Low-dose vaginal estrogen is a different, lower-risk category than systemic estrogen. It treats vaginal and urinary symptoms with much less estrogen reaching the bloodstream, and it hasn’t been shown to raise endometrial cancer risk. Across 20 randomized trials involving 2,983 women, reported endometrial cancer and hyperplasia rates were about 0.03% and 0.4%. A progestogen generally isn’t recommended alongside it. [7][8]
"Vaginal" doesn't automatically mean "low-dose local"
Estring is a low-dose local ring for vaginal symptoms. Femring is a systemic ring used for hot flashes and night sweats — it raises estrogen body-wide and carries the same systemic warnings. [16] Same body part, very different exposure. Confirm your exact product.
Most of the safety evidence is short-term
The trials above generally ran up to a year, so longer-term randomized data are limited. Low-risk is not the same as proven zero risk.
Any bleeding after menopause still gets checked
Even on vaginal estrogen. Bleeding is a symptom, not something to explain away.
If vaginal symptoms are your main concern, our full guide to vaginal estrogen for menopause covers products, differences, and how to get a prescription.
Can I just get regular ultrasounds or biopsies instead of taking progesterone?
No. Monitoring can only look for changes after they start — it can’t preventthe overgrowth that unopposed estrogen causes, and it isn’t a substitute for a clinician-directed protection plan. There’s also no routine screening test for endometrial cancer in average-risk women without symptoms, and a Pap test screens for cervical cancer, not endometrial cancer. [17]
| Endometrial protection (progestogen, IUD, or combined product) | Monitoring (ultrasound / biopsy) |
|---|---|
| Reduces harmful stimulation before problems develop | Investigates symptoms or changes after they appear |
| Part of your treatment plan | Part of a workup when something's wrong |
| A normal past scan doesn't replace it | A normal past scan doesn't guarantee the future |
A thin lining on ultrasound is reassuring, but it’s a snapshot, not a permanent guarantee. As of , ACOG updated its bleeding guidance — see the bleeding section below for details. Monitoring is a tool for evaluating symptoms, not a replacement for protection.
What if I can’t tolerate progesterone?
Simply dropping your endometrial protection while staying on systemic estrogen is not a safe do-it-yourself fix if you have a uterus. But you’re not stuck — a clinician can often switch the progestogen, the route, the schedule, or the whole approach. Progestogen side effects (mood changes, bloating, fatigue, breast tenderness) are a common reason women want to quit, and they deserve a real solution.
Things a clinician might consider
- A different progestogen (some are tolerated better than others)
- A hormonal IUD that delivers progestogen locally to the lining
- A different schedule, or a lower or different estrogen dose
- A progestogen-free protective combination (conjugated estrogens with bazedoxifene)
- Local vaginal treatment instead of systemic, if your main symptoms are genitourinary
- Non-hormonal options for hot flashes
What not to do
- Skip doses
- Swap in an over-the-counter progesterone cream as a substitute
- Cut or boost your own estrogen
- Rely on an annual scan as “coverage”
Bring to your visit
Exactly which side effect you get, when it hits after each dose, what you’ve already tried, your current dose and schedule, whether you need estrogen for whole-body or just local symptoms, and any bleeding.
Struggling with your current regimen?We’ll help point you to the right kind of care so the conversation gets to a real fix faster — without you having to guess at the medicine.
See which care path fits when progesterone is hard to tolerate →What bleeding on HRT needs to be checked — and what changed in 2026
Bleeding after menopause is the single most important symptom to get evaluated, because about 90% of endometrial cancers show up as postmenopausal bleeding. [18] The good news: most bleeding isn’t cancer — about 9% of women evaluated for postmenopausal bleeding are diagnosed with endometrial cancer, and lining thinning (atrophy) is the most common cause. [19]
The safe rule
Postmenopausal bleeding (bleeding 12 or more months after your last period) should be reported when it happens — including after starting or changing HRT. A scheduled monthly bleed on cyclical HRT is different and expected; your prescriber should tell you what’s normal for your regimen. Anything unscheduled, heavy, recurrent, or worrying is a reason to call. [20] See also: our full bleeding after starting HRT guide and spotting on HRT.
Write down before you call
When it started, how heavy, how long, whether it keeps returning, whether it followed a medication or dose change, your last natural period, your HRT products and schedule, any missed doses, and any pain or other symptoms.
What changed in — why some older pages are now out of date
ACOG updated its guidance on evaluating postmenopausal bleeding. For most patients, it now recommends both a transvaginal ultrasound and an endometrial biopsy at the first evaluation — instead of the older approach of ultrasound alone when the lining measured 4 mm or less. [20] The reason: endometrial cancer has been rising, and ultrasound alone can miss an estimated 5 to 12% of cancers at first check.
Ultrasound without a biopsy may still be reasonable for a select patient with a single bleeding episode, a fully visualized lining no thicker than 4 mm, no major risk factors, and prompt access to care. [20] If your last workup was ultrasound-only, this is worth knowing.
What the FDA’s 2025–2026 warning changes mean for you
In the FDA began removing several risk statements from the boxed warnings on menopause hormone products — but it deliberately kept the boxed warning about endometrial cancer for systemic estrogen-alone products used by women with a uterus. [21][22][23]
| Date | What happened |
|---|---|
| HHS and the FDA announced they would remove boxed-warning statements about cardiovascular disease, breast cancer, and probable dementia from estrogen-containing menopause products, citing newer evidence and benefits when therapy starts within about 10 years of menopause. [21] | |
| FDA approved the first batch of six products with updated labels: Bijuva, Divigel, Cenestin, Enjuvia, Prometrium, and Estring; 29 manufacturers had submitted proposed changes. [22] |
What changed
The risk statements about cardiovascular disease, breast cancer, and probable dementia were removed from the boxed warning. Some of that risk information still appears elsewhere in the prescribing information.
What was kept — and why it matters for this page
The FDA explicitly stated it is not removing the boxed warning for endometrial cancer for systemic estrogen-alone products. [21][23] The Society of Gynecologic Oncology underscored the same point. [23]
Read the change carefully: even while pulling back warnings it considered overstated, the FDA left this onein place. That’s not a loophole — it’s a signal that the estrogen-and-the-lining risk is the one regulators still want front and center. If you have a uterus and use systemic estrogen, you still need protection.
Who has a higher baseline risk of endometrial cancer?
HRT is only one piece of endometrial cancer risk. Age, extra body weight, diabetes, PCOS, never having been pregnant, certain inherited syndromes, and tamoxifen all factor in. Body weight is one of the biggest: one large analysis found women who are overweight had about 1.4 times the odds, and women with obesity about 3.3 times the odds, compared with women at a normal weight — because fat tissue itself makes estrogen. [24]
| Factor | Why it matters to the conversation | What it does not mean |
|---|---|---|
| Extra body weight / metabolic syndrome | Body fat produces estrogen, which can raise baseline risk | It doesn't diagnose cancer or decide whether HRT is right for you |
| Diabetes, high blood pressure, PCOS | Linked to higher endometrial risk | One risk factor isn't a diagnosis or a personal percentage |
| Lynch syndrome (an inherited condition) | Can meaningfully change screening and specialist planning | A general HRT page can't manage inherited-cancer risk |
| Tamoxifen (a breast cancer medication) | Raises endometrial risk; report any abnormal bleeding promptly | It isn't a reason for routine ultrasound screening if you have no symptoms |
| Family history of uterine/colon cancer | May justify a fuller history or genetic counseling | One affected relative doesn't give you a number |
If you carry higher baseline risk, that’s more reason to confirm your HRT includes an evidence-supported, clinician-directed protection plan — not a reason to fear estrogen across the board.
Can HRT cause endometrial hyperplasia before cancer?
Yes — unopposed estrogen can cause endometrial hyperplasia, meaning the lining overgrows. The milder form is not the same as cancer and rarely progresses, but it needs a clinician to diagnose and manage. Endometrial hyperplasia without atypia has a low chance of becoming cancer — fewer than 5 in 100 women develop endometrial cancer over 20 years, and roughly 7 to 8 in 10 cases regress without treatment. [25]
Overgrowth with normal-looking cells. Lower concern; often managed with a progestogen and follow-up.
Overgrowth with abnormal cells. More concerning, and handled by a specialist. The figures above do not apply to this category.
Not a diagnosis by itself. It's a reason to look closer, not a verdict.
Can I take HRT after endometrial hyperplasia or endometrial cancer?
A history of hyperplasia, atypical hyperplasia/EIN, or endometrial cancer moves this out of ordinary online-HRT territory and into individualized specialist care. The answer depends on your exact pathology, stage, prior treatment, remaining anatomy, how long ago it was, your symptoms, and whether the therapy would be systemic or local — which is why a general page (or a general telehealth intake) can’t and shouldn’t decide it.
Questions for your gynecologist or oncology team
- What exactly was my pathology and stage?
- Do I still have a uterus?
- Is the symptom I want treated local (vaginal) or whole-body?
- What non-hormonal options make sense for me?
- Would low-dose local treatment be considered differently from systemic HRT?
- Who coordinates my follow-up?
If this is you, start with a gynecologist or gynecologic oncologist — not a generic provider match.
How to check that an online HRT provider actually protects your endometrium
A trustworthy provider confirms whether you have a uterus, tells you plainly whether your medications are FDA-approved or compounded, spells out exactly what protects your lining, explains what bleeding to report and to whom, and refers complex histories to in-person care. Labels like “bioidentical,” “natural,” or “personalized” don’t, on their own, establish FDA approval, manufacturing consistency, or adequate endometrial protection.
The HRT Index Verification Standard — five pillars applied to your endometrial safety:
Clinical legitimacy
Is a licensed clinician actually involved and licensed in your state? Do they screen for cancer history and contraindications? Do they confirm your uterus/hysterectomy/ablation status? Is there a clear path if you bleed, and a referral route for a complicated history?
Care quality
Does a real clinician review your intake — or is it a form and a rubber stamp? How do you reach them for follow-up or side effects? Who evaluates bleeding? Do medication changes trigger a proper reassessment?
Medication fit
Is your estrogen systemic or local? Is each medication FDA-approved or compounded — stated clearly, not blurred? What's the exact progestogen plan? What happens if you can't tolerate it? Are vaginal-only symptoms treated differently from whole-body symptoms?
Price transparency
Does the quoted price include the clinician visit? Are medication, labs, or any needed evaluation extra? Does escalating to in-person care add cost? Can they bill insurance? Confirm the current price at intake or checkout.
Access
Are they available in your state? How fast can you be seen? Can they refer you in-person or coordinate an evaluation if bleeding comes up? Can records and prescriptions transfer?
Ten questions to ask before you pay
- Is my estrogen systemic or low-dose local?
- How did you confirm whether I still have a uterus?
- What exactly protects my uterine lining?
- Is each medication FDA-approved or compounded?
- Why does this progestogen route and schedule fit my estrogen?
- What happens if I can’t tolerate it?
- What bleeding should I report, and to whom?
- Can your service order or coordinate an endometrial evaluation?
- What history would make you refer me to in-person care?
- What costs are not included if I need extra evaluation?
Wondering if online care even makes sense for your situation? Our tool matches your symptoms, anatomy, and history to the right kind of care — and flags when you should begin with an in-person clinician.
Check whether online care is the right starting point for you →The bottom line for your exact situation
Call your prescriber and ask what protects your lining. Don't assume a patch or "low dose" solves it. Don't stop anything on your own.
Confirm the exact progestogen, route, schedule, and how consistently you take it — and what happens after any estrogen-dose change.
Confirm it was total, and that no history changes the usual rule. Then this risk mostly isn't yours.
Get your operative or pathology report — and remember an ablation doesn't remove the need for protection with systemic estrogen.
Confirm the exact product and that it's truly local (Estring is; Femring isn't); see our vaginal estrogen guide for the full picture. Report any bleeding.
Ask about alternatives — don't drop protection while staying on systemic estrogen.
Contact a clinician promptly. Don't wait for a quiz result.
Start with a gynecologist or gynecologic oncologist.
How we researched and verified this guide
What we verified
- The FDA’s and label changes — including that the endometrial-cancer boxed warning was kept for systemic estrogen-alone products
- ACOG’s guidance that adding a progestogen lowers the risk from estrogen-only therapy
- ACOG’s update on evaluating postmenopausal bleeding
- The exact Women’s Health Initiative combined-therapy regimen and its reported endometrial cancer numbers
- The current U.S. label status of Mirena, Femring, Estring, and DUAVEE
- Current menopause-society and cancer-organization guidance on compounded hormones, vaginal estrogen, hyperplasia, and risk factors
What we did not verify (and can’t)
Whether your specific regimen is right for you · whether a specific dose protects your lining · the cause of any bleeding · your personal cancer risk · how any individual provider would handle your case.
Last verified: · Written by The HRT Index Editorial Team · Independent editorial research, not reviewed by a clinician · The HRT Index Verification Standard
| Date | What changed |
|---|---|
| Initial publication. FDA (Nov 2025 / Feb 2026 label changes), ACOG (incl. April 2026 bleeding update), WHI, U.S. product labels (Mirena, Femring, Estring, DUAVEE), and cancer-organization sources verified. |
Editorial research — not medically reviewed. This is general information, not medical advice. Talk with your own clinician before starting, stopping, or changing hormone therapy.
Frequently asked questions
The same rule throughout: your anatomy, your exact regimen, your history, and your clinician’s assessment are the only way to know what’s right for you.
Still deciding?
Still not sure which HRT program is right for you?Take our free matching quiz — it takes about 90 seconds. It helps you find the care pathway that fits your situation, and it flags when online care isn’t the right starting point. It doesn’t diagnose bleeding, calculate cancer risk, or replace a clinician.
Take the free matching quiz (~90 seconds) →Sources
- ACOG. Hormone Therapy for Menopause (patient FAQ) — estrogen-alone therapy thickens the uterine lining and increases endometrial cancer risk; adding progestin decreases that risk. acog.org. Accessed .
- U.S. Food and Drug Administration. Class labeling for systemic estrogen products (boxed warning, “Endometrial Cancer”) — reported risk about 2–12× non-users; 15–24× after 5–10+ years; persistence after discontinuation. DailyMed. Accessed .
- British Menopause Society. Tools for Clinicians: Progestogens and Endometrial Protection () — progestogen duration; 52 mg levonorgestrel IUS; combined HRT after ablation; compounded transdermal progesterone concerns. thebms.org.uk. Accessed .
- Chlebowski RT, Anderson GL, Sarto GE, et al. Continuous Combined Estrogen Plus Progestin and Endometrial Cancer: The Women’s Health Initiative Randomized Trial. J Natl Cancer Inst. 2016;108(3):djv350. PMID 26668177.
- Mirena (levonorgestrel-releasing intrauterine system) U.S. Prescribing Information — indicated for contraception and heavy menstrual bleeding; no menopausal-HRT/endometrial-protection indication. Bayer / DailyMed. Accessed .
- DUAVEE (conjugated estrogens/bazedoxifene) U.S. Prescribing Information — “the bazedoxifene component reduces the risk of endometrial hyperplasia that can occur with the conjugated estrogens component.” Pfizer / DailyMed. Accessed .
- Constantine GD, et al. Endometrial safety of low-dose vaginal estrogens in menopausal women: a systematic review. Menopause. 2019;26(7):800–807. PMC6636806.
- The Menopause Society. Hormone therapy guidance — a progestogen is not recommended with low-dose vaginal estrogen. menopause.org. Accessed .
- U.S. FDA — systemic estrogen-alone therapy is typically used in women without a uterus (after hysterectomy). DailyMed. Accessed .
- Eden JA, et al. Case series of endometrial cancers in women using compounded “bioidentical” hormone therapy. (Case report evidence, not a class-wide incidence.) PubMed. Accessed .
- U.S. FDA. Compounding and the FDA: Questions and Answers — compounded drugs are not FDA-approved; FDA does not verify their safety, effectiveness, or quality before marketing. fda.gov. Accessed .
- ACOG. Postmenopausal Estrogen Therapy: Route of Administration and Risk of Venous Thromboembolism (Committee Opinion) — transdermal estrogen associated with lower VTE risk than oral. acog.org. Accessed .
- McBane SE, et al. Analysis of compounded hormone products — variability in active-ingredient content. PubMed PMID 31453957. Accessed .
- The Menopause Society — compounded hormones not recommended for menopause symptoms when FDA-approved options exist. menopause.org. Accessed .
- Estring (estradiol vaginal ring) U.S. Prescribing Information — low-dose local product; systemic absorption generally lower than systemic products. DailyMed. Accessed .
- Femring (estradiol acetate vaginal ring) U.S. Prescribing Information — systemic ring for moderate-to-severe vasomotor symptoms; carries the systemic boxed warning. DailyMed. Accessed .
- American Cancer Society. Can Endometrial Cancer Be Found Early? — no routine screening test for average-risk women; Pap tests are not effective endometrial cancer screening. cancer.org. Accessed .
- ACOG — approximately 90% of endometrial cancers present with postmenopausal bleeding. acog.org. Accessed .
- National Cancer Institute. For Postmenopausal Bleeding, Prompt Follow-up Is Advised — roughly 9% of women with postmenopausal bleeding are diagnosed with endometrial cancer. cancer.gov. Accessed .
- ACOG. Updated Guidance Regarding the Role of Transvaginal Ultrasonography in Evaluating the Endometrium of Individuals With Postmenopausal Bleeding (Clinical Practice Update, ). Obstet Gynecol. 2026.
- U.S. FDA / HHS. HHS Advances Women’s Health, Removes Misleading FDA Warnings on Hormone Replacement Therapy () — endometrial-cancer boxed warning for systemic estrogen-alone products NOT removed. fda.gov / hhs.gov.
- U.S. FDA. FDA Approves Labeling Changes to Menopausal Hormone Therapy Products () — first batch of six products. fda.gov.
- Society of Gynecologic Oncology. Statement on FDA boxed-warning changes — endometrial-cancer warning remains for systemic estrogen-alone therapy in women with a uterus. sgo.org (). Accessed .
- Meta-analysis of body mass index and endometrial cancer — odds ratios ~1.43 (overweight) and ~3.33 (obesity) versus normal weight. PubMed PMID 26026348. Accessed .
- Royal College of Obstetricians and Gynaecologists. Endometrial Hyperplasia (patient information) — fewer than 5 in 100 women with hyperplasia without atypia develop endometrial cancer over 20 years. rcog.org.uk. Accessed .
This guide is editorial research and is not medical advice. It was not reviewed by a clinician. Always talk with your own clinician before starting, stopping, or changing hormone therapy. Do not start, stop, or change HRT based on a table or article.